Solumsmoen Stian, Poulsen Gry, Kjellberg Jakob, Melbye Mads, Munch Tina Nørgaard
Copenhagen Spine Research Unit (CSRU), Section of Spine Surgery, Center of Rheumatology and Spine Diseases, Rigshospitalet Glostrup, Valdemar Hansens vej 17, Glostrup 2600, Denmark.
Department of Epidemiology Research, Statens Serum Institut, Copenhagen, Denmark.
EClinicalMedicine. 2021 Dec 24;43:101247. doi: 10.1016/j.eclinm.2021.101247. eCollection 2022 Jan.
Low back pain (LBP) is the most common diagnosis responsible for sick leave, long-term disability payments, and early retirements. Studies have suggested that the relatively small proportion of patients referred to a specialist for treatment, either conservative or surgical, accounts for most of the total costs of back pain. However, a complete and long-term picture of the socioeconomic burden associated with these two treatment regimens is lacking.
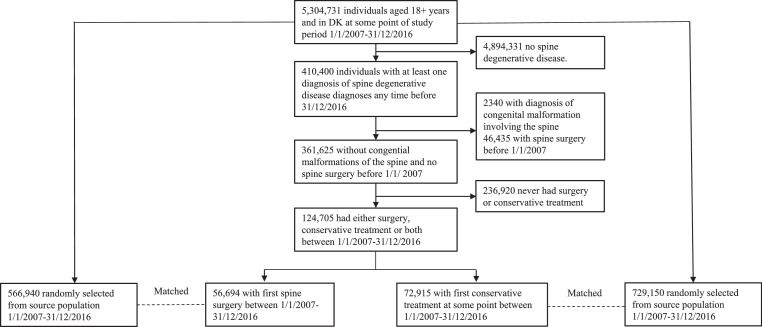
From a cohort encompassing the entire population in Denmark (5.8 million inhabitants), we identified patients with LBP referred to specialised treatment, either conservative or surgical, during 2007-2016. According to treatment modality, two different cohorts were constructed. Each patient was matched with ten background population controls based on age, sex, region of residency and time of treatment (month and year). Using extensive, nationwide register data, the healthcare costs and loss of productivity from two years before the first intervention until 2018 was investigated.
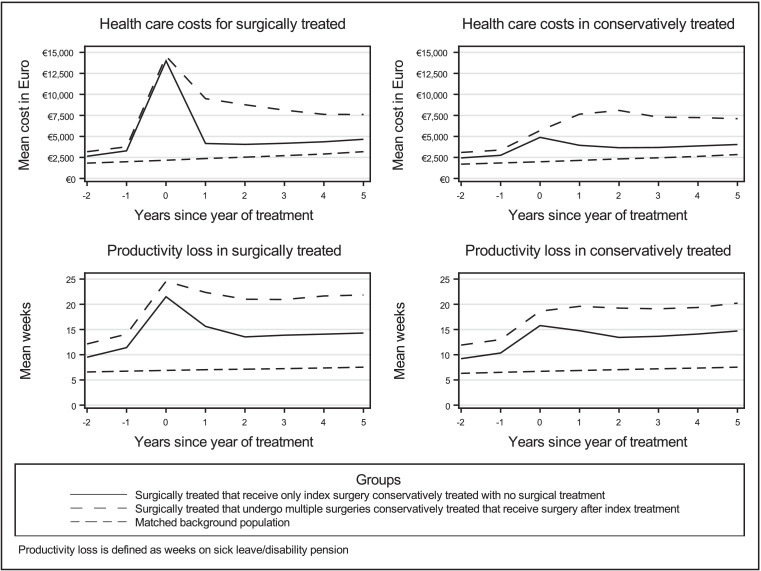
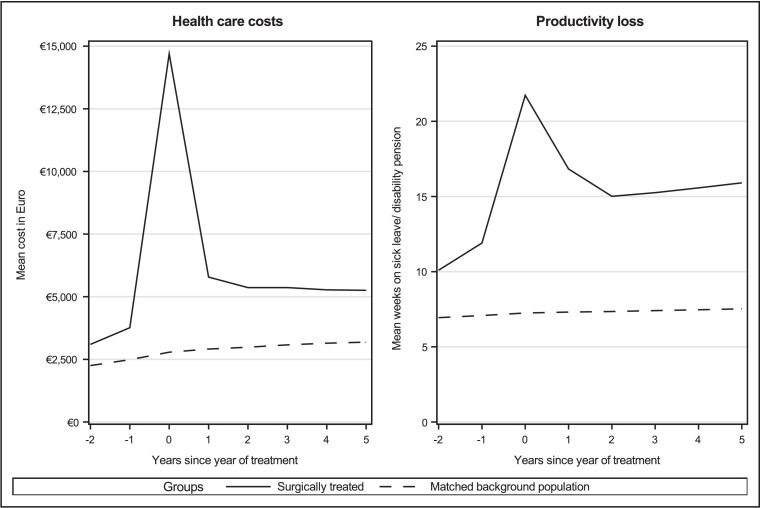
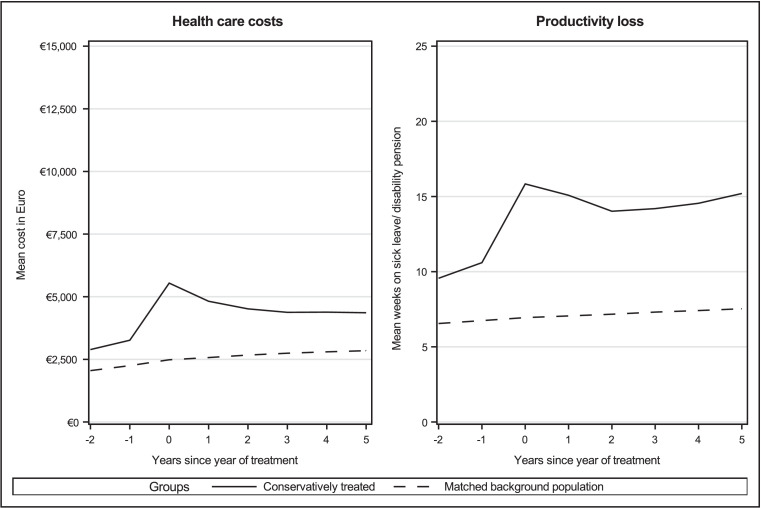
A total of 56,694 patients underwent surgical treatment, and 72,915 patients conservative treatment. Both cohorts had a significantly higher baseline cost two years before treatment compared with the background population controls. These measures increased sharply during the year after treatment. Five years after treatment, healthcare costs and loss of productivity remained proportionally similarly increased for the two treatment groups compared to the background population. Multiple surgeries had detrimental effects on long term productivity for the patients, and spouses to patients had marginally increased loss of productivity.
The results show that patients referred to specialised treatment of LBP display poor socioeconomic prognosis, regardless of conservative or surgical treatment modality. This development was reinforced in patients undergoing multiple surgeries and was also observed among spouses to the patients. Our findings of substantial loss of productivity across subgroups indicate that measures of successful treatment need to be more nuanced.
腰痛是导致病假、长期残疾津贴和提前退休的最常见诊断原因。研究表明,转诊至专科医生处接受保守或手术治疗的患者比例相对较小,但却占了背痛总成本的大部分。然而,目前缺乏与这两种治疗方案相关的社会经济负担的完整长期情况。
从涵盖丹麦全体人口(580万居民)的队列中,我们识别出在2007年至2016年期间转诊至专科接受保守或手术治疗的腰痛患者。根据治疗方式构建了两个不同的队列。每位患者根据年龄、性别、居住地区和治疗时间(月份和年份)与十名背景人群对照进行匹配。利用广泛的全国登记数据,调查了从首次干预前两年到2018年的医疗费用和生产力损失情况。
共有56,694名患者接受了手术治疗,72,915名患者接受了保守治疗。与背景人群对照相比,两个队列在治疗前两年的基线成本均显著更高。这些指标在治疗后的一年内急剧上升。治疗五年后,与背景人群相比,两个治疗组的医疗费用和生产力损失仍按比例类似地增加。多次手术对患者的长期生产力有不利影响,患者配偶的生产力损失略有增加。
结果表明,转诊至腰痛专科治疗的患者,无论采用保守还是手术治疗方式,其社会经济预后都较差。这种情况在接受多次手术的患者中更为明显,在患者配偶中也有观察到。我们在各亚组中发现的大量生产力损失表明,成功治疗的衡量标准需要更加细致入微。