Matsui Masahiro, Nishikawa Hiroki, Goto Masahiro, Asai Akira, Ushiro Kosuke, Ogura Takeshi, Takeuchi Toshihisa, Nakamura Shiro, Kakimoto Kazuki, Miyazaki Takako, Fukunishi Shinya, Ohama Hideko, Yokohama Keisuke, Yasuoka Hidetaka, Higuchi Kazuhide
The Second Department of Internal Medicine, Osaka Medical and Pharmaceutical University, Takatsuki 569-8686, Japan.
The Premier Departmental Research of Medicine, Osaka Medical and Pharmaceutical University, Takatsuki 569-8686, Japan.
Cancers (Basel). 2021 Dec 21;14(1):10. doi: 10.3390/cancers14010010.
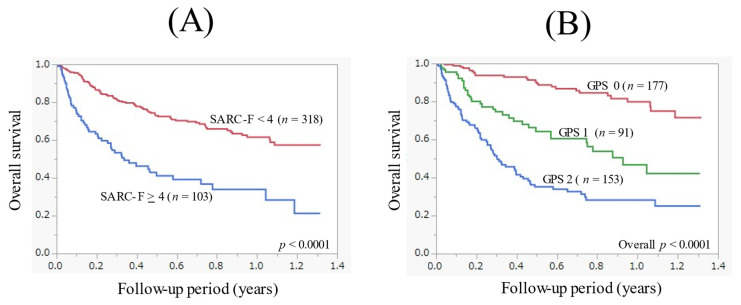
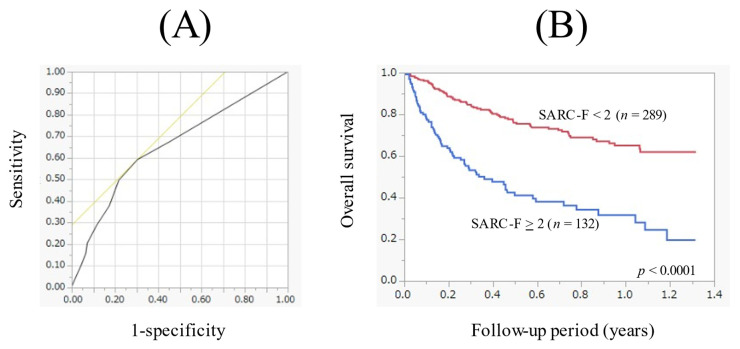
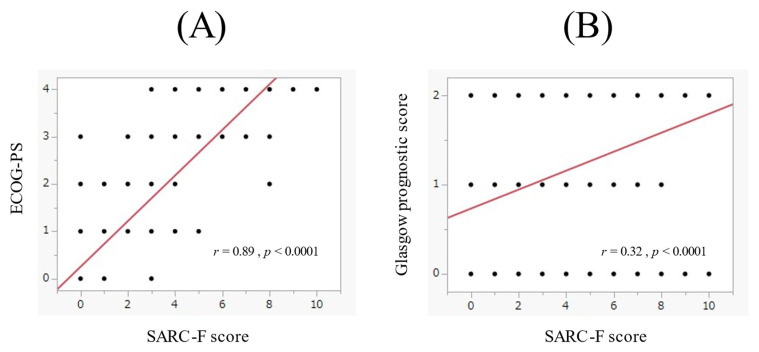
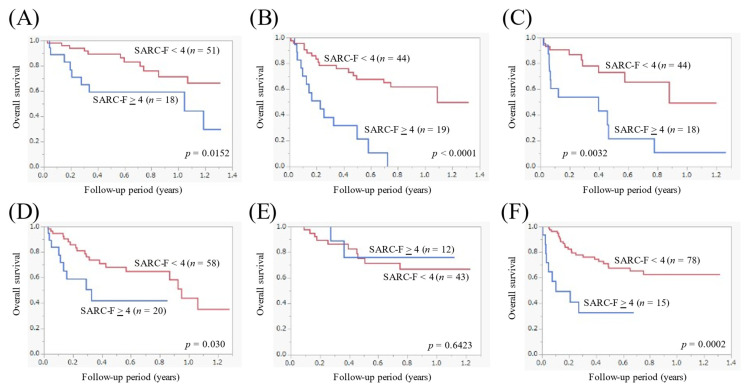
We sought to elucidate the prognostic impact of the SARC-F score among patients with gastrointestinal advanced malignancies ( = 421). A SARC-F score ≥ 4 was judged to have a strong suspicion for sarcopenia. In patients with ECOG-PS 4 ( = 43), 3 ( = 61), and 0-2 ( = 317), 42 (97.7%), 53 (86.9%) and 8 (2.5%) had the SARC-F score ≥ 4. During the follow-up period, 145 patients (34.4%) died. All deaths were cancer-related. The 1-year cumulative overall survival (OS) rate in patients with SARC-F ≥ 4 ( = 103) and SARC-F < 4 ( = 318) was 33.9% and 61.6% ( < 0.0001). In the multivariate analysis for the OS, total lymphocyte count ≥ 1081/μL ( = 0.0014), the SARC-F score ≥ 4 ( = 0.0096), Glasgow prognostic score (GPS) 1 ( = 0.0147, GPS 0 as a standard), GPS 2 ( < 0.0001, GPS 0 as a standard), ECOG-PS 2 ( < 0.0001, ECOG-PS 0 as a standard), ECOG-PS 3 ( < 0.0001, ECOG-PS 0 as a standard), and ECOG-PS 4 ( < 0.0001, ECOG-PS 0 as a standard) were independent predictors. In the receiver operating characteristic curve analysis on the prognostic value of the SARC-F score, the sensitivity/specificity was 0.59/0.70, and best cutoff point of the SARC-F score was two. In conclusion, the SARC-F score is useful in patients with gastrointestinal advanced malignancies.
我们试图阐明SARC - F评分对胃肠道晚期恶性肿瘤患者(n = 421)的预后影响。SARC - F评分≥4被判定为高度怀疑存在肌肉减少症。在东部肿瘤协作组(ECOG)体能状态评分为4(n = 43)、3(n = 61)和0 - 2(n = 317)的患者中,SARC - F评分≥4的分别有42例(97.7%)、53例(86.9%)和8例(2.5%)。在随访期间,145例患者(34.4%)死亡。所有死亡均与癌症相关。SARC - F≥4(n = 103)和SARC - F < 4(n = 318)患者的1年累积总生存率(OS)分别为33.9%和61.6%(P < 0.0001)。在OS的多因素分析中,总淋巴细胞计数≥1081/μL(P = 0.0014)、SARC - F评分≥4(P = 0.0096)、格拉斯哥预后评分(GPS)为1(P = 0.0147,以GPS 0为标准)、GPS为2(P < 0.0001,以GPS 0为标准)、ECOG - PS为2(P < 0.0001,以ECOG - PS 0为标准)、ECOG - PS为3(P < 0.0001,以ECOG - PS 0为标准)以及ECOG - PS为4(P < 0.0001,以ECOG - PS 0为标准)是独立的预测因素。在对SARC - F评分预后价值的受试者工作特征曲线分析中,敏感度/特异度为0.59/0.70,SARC - F评分的最佳截断点为2。总之,SARC - F评分对胃肠道晚期恶性肿瘤患者有用。