Aleksandric Srdjan B, Djordjevic-Dikic Ana D, Giga Vojislav L, Tesic Milorad B, Soldatovic Ivan A, Banovic Marko D, Dobric Milan R, Vukcevic Vladan, Tomasevic Miloje V, Orlic Dejan N, Boskovic Nikola, Jovanovic Ivana, Nedeljkovic Milan A, Stankovic Goran, Ostojic Miodrag C, Beleslin Branko D
Cardiology Clinic, University Clinical Center of Serbia, 11000 Belgrade, Serbia.
Faculty of Medicine, University of Belgrade, 11000 Belgrade, Serbia.
J Clin Med. 2021 Dec 30;11(1):204. doi: 10.3390/jcm11010204.
It has been shown that coronary flow velocity reserve (CFVR) measurement by transthoracic Doppler echocardiography (TTDE) during dobutamine (DOB) provocation provides a more accurate functional evaluation of myocardial bridging (MB) compared to adenosine. However; the cut-off value of CFVR during DOB for identification of MB associated with myocardial ischemia has not been fully clarified.
This prospective study aimed to determine the cut-off value of TTDE-CFVR during DOB in patients with isolated-MB, as compared with stress-induced wall motion abnormalities (VMA) during exercise stress-echocardiography (SE) as reference.
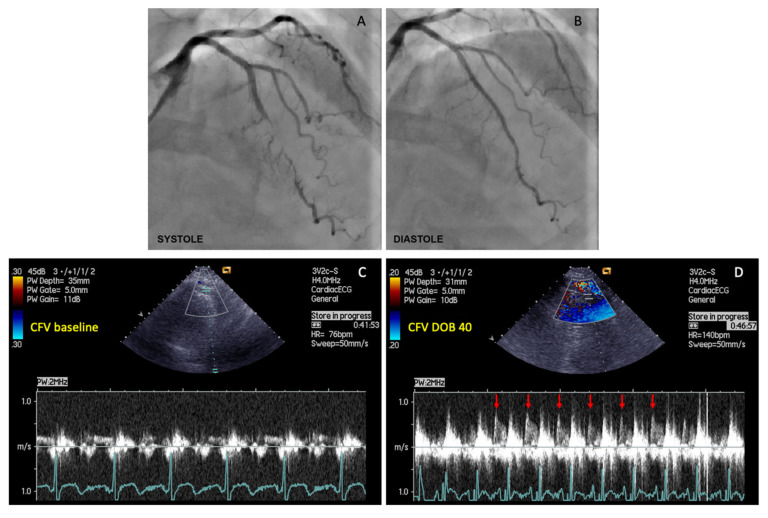
Eighty-one symptomatic patients (55 males [68%], mean age 56 ± 10 years; range: 27-74 years) with the existence of isolated-MB on the left anterior descending artery (LAD) and systolic MB-compression ≥50% diameter stenosis (DS) were eligible to participate in the study. Each patient underwent treadmill exercise-SE, invasive coronary angiography, and TTDE-CFVR measurements in the distal segment of LAD during DOB infusion (DOB: 10-40 μg/kg/min). Using quantitative coronary angiography, both minimal luminal diameter (MLD) and percent DS at MB-site at end-systole and end-diastole were determined.
Stress-induced myocardial ischemia with the occurrence of WMA was found in 23 patients (28%). CFVR during peak DOB was significantly lower in the SE-positive group compared with the SE-negative group (1.94 ± 0.16 vs. 2.78 ± 0.53; < 0.001). ROC analyses identified the optimal CFVR cut-off value ≤ 2.1 obtained during high-dose dobutamine (>20 µg/kg/min) for the identification of MB associated with stress-induced WMA, with a sensitivity, specificity, positive and negative predictive value of 96%, 95%, 88%, and 98%, respectively (AUC 0.986; 95% CI: 0.967-1.000; < 0.001). Multivariate logistic regression analysis revealed that MLD and percent DS, both at end-diastole, were the only independent predictors of ischemic CFVR values ≤2.1 (OR: 0.023; 95% CI: 0.001-0.534; = 0.019; OR: 1.147; 95% CI: 1.042-1.263; = 0.005; respectively).
Noninvasive CFVR during dobutamine provocation appears to be an additional and important noninvasive tool to determine the functional severity of isolated-MB. A transthoracic CFVR cut-off ≤2.1 measured at a high-dobutamine dose may be adequate for detecting myocardial ischemia in patients with isolated-MB.
经胸多普勒超声心动图(TTDE)在多巴酚丁胺(DOB)激发试验期间测量冠状动脉血流速度储备(CFVR),与腺苷相比,能为心肌桥(MB)提供更准确的功能评估。然而,DOB激发试验期间CFVR用于识别与心肌缺血相关的MB的临界值尚未完全明确。
本前瞻性研究旨在确定孤立性MB患者在DOB激发试验期间TTDE-CFVR的临界值,并与运动负荷超声心动图(SE)期间的应激性室壁运动异常(VMA)作为参考进行比较。
81例有症状患者(55例男性[68%],平均年龄56±10岁;范围:27 - 74岁),左前降支(LAD)存在孤立性MB且收缩期MB压迫导致管腔直径狭窄(DS)≥50%,符合纳入本研究条件。每位患者均接受平板运动-SE、有创冠状动脉造影以及在输注DOB(DOB:10 - 40μg/kg/min)期间对LAD远端节段进行TTDE-CFVR测量。使用定量冠状动脉造影,测定收缩末期和舒张末期MB部位的最小管腔直径(MLD)和DS百分比。
23例患者(28%)出现应激性心肌缺血并伴有室壁运动异常。SE阳性组在DOB峰值时的CFVR显著低于SE阴性组(1.94±0.16 vs. 2.78±0.53;P<0.001)。ROC分析确定在高剂量多巴酚丁胺(>20μg/kg/min)期间获得的CFVR临界值≤2.1可用于识别与应激性室壁运动异常相关的MB,其敏感性为分别为96%、95%、88%和98%(AUC 0.986;95% CI:0.967 - 1.000;P<0.001)。多因素逻辑回归分析显示,舒张末期的MLD和DS百分比是缺血性CFVR值≤2.1的唯一独立预测因素(OR:0.023;95% CI:0.001 - 0.534;P = 0.019;OR:1.147;95% CI:1.042 - 1.263;P = 0.005)。
多巴酚丁胺激发试验期间的无创CFVR似乎是确定孤立性MB功能严重程度的一种额外且重要的无创工具。高剂量多巴酚丁胺时经胸CFVR临界值≤2.1可能足以检测孤立性MB患者的心肌缺血。