Department of Thoracic Surgery, West China Hospital, Sichuan University, Chengdu, China.
West China School of Medicine, Sichuan University, Chengdu, China.
Interact Cardiovasc Thorac Surg. 2022 May 2;34(5):744-752. doi: 10.1093/icvts/ivab350.
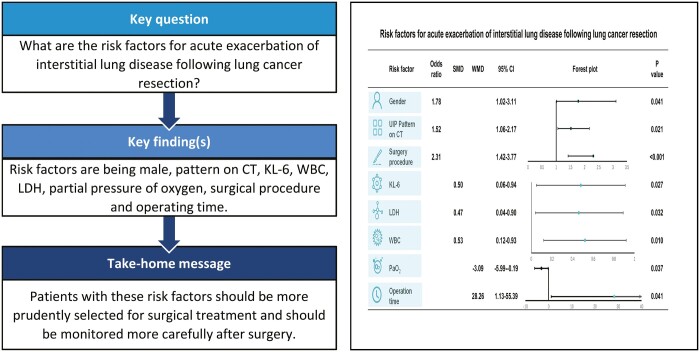
The aim of this study was to investigate the risk factors for acute exacerbation (AE) of interstitial lung disease (ILD) following lung cancer resection.
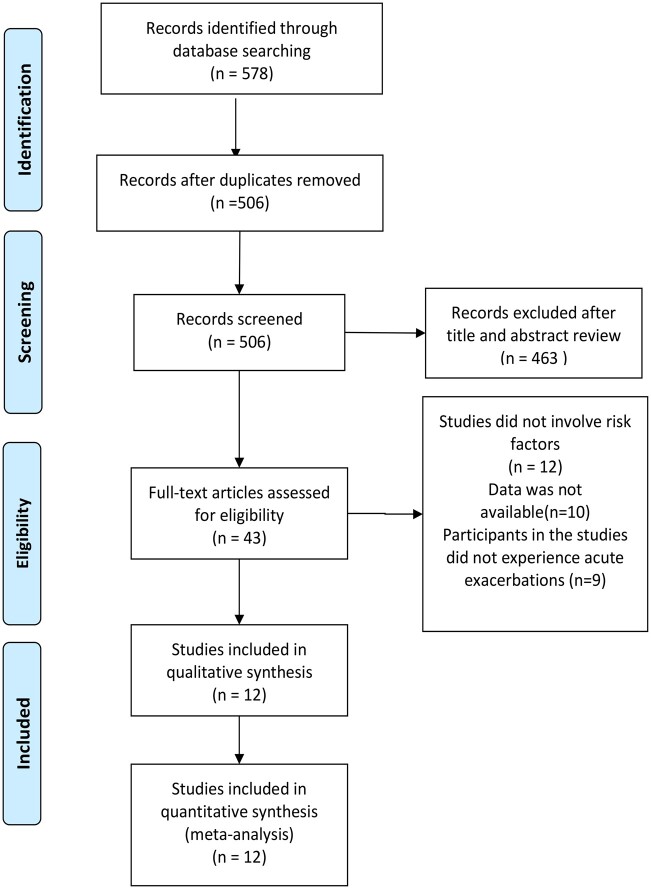
We performed a literature screening on the databases including PubMed, Embase, Ovid MEDLINE® and the Web of Science for related studies published up to January 2021. Eligible studies were included and data on risk factors related to postoperative AE were extracted. All analyses were performed with random-effect model.
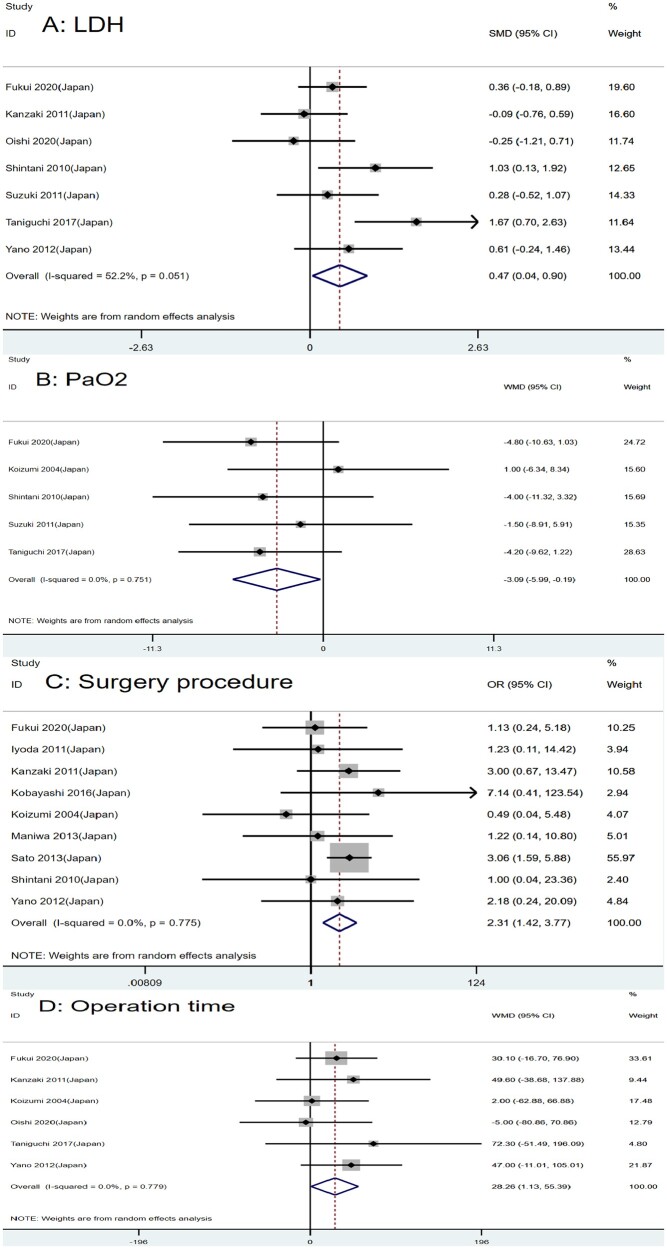
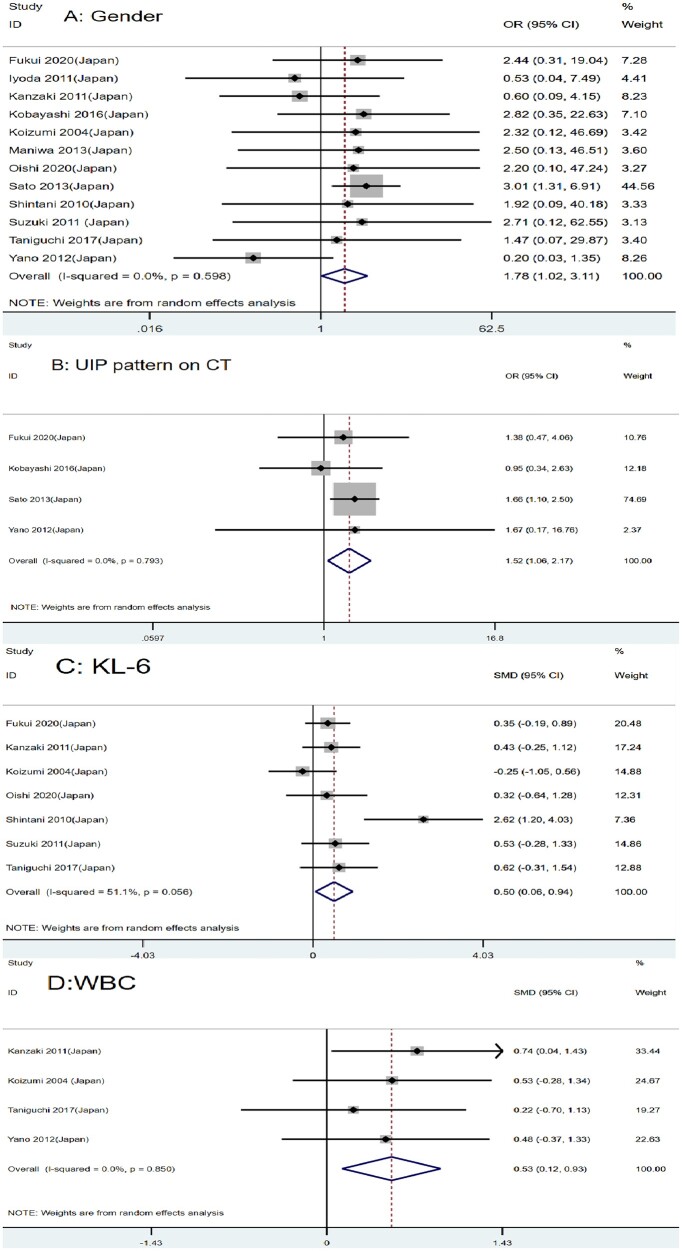
A total of 12 studies of 2655 lung cancer patients with ILD were included in this article. The meta-analysis indicated that male [odds ratios (ORs) = 1.78, 95% confidence interval (CI): 1.02-3.11, P = 0.041], usually interstitial pneumonia pattern on CT (OR = 1.52, 95% CI: 1.06-2.17, P = 0.021), Krebs von den Lungen-6 [standardized mean difference (SMD) = 0.50, 95% CI: 0.06-0.94, P = 0.027], white blood cell (SMD = 0.53, 95% CI: 0.12-0.93, P = 0.010), lactate dehydrogenase (SMD = 0.47, 95% CI: 0.04-0.90, P = 0.032), partial pressure of oxygen (weighted mean difference = -3.09, 95% CI: -5.99 to -0.19, P = 0.037), surgery procedure (OR = 2.31, 95% CI: 1.42-3.77, P < 0.001) and operation time (weighted mean difference = 28.26, 95% CI: 1.13-55.39, P = 0.041) were risk factors for AE of ILD following lung cancer resection.
We found that males, usually interstitial pneumonia pattern on CT, higher levels of Krebs von den Lungen-6, lactate dehydrogenase, white blood cell, lower partial pressure of oxygen, greater scope of operation and longer operation time were risk factors for AE of ILD following lung cancer resection. Patients with these risk factors should be more prudently selected for surgical treatment and be monitored more carefully after surgery.
本研究旨在探讨肺癌切除术后间质性肺病(ILD)急性加重(AE)的危险因素。
我们在 PubMed、Embase、Ovid MEDLINE®和 Web of Science 数据库中进行了文献筛选,纳入了截至 2021 年 1 月发表的与术后 AE 相关的研究。纳入符合条件的研究,并提取与术后 AE 相关的危险因素数据。所有分析均采用随机效应模型进行。
本文共纳入了 12 项研究的 2655 例肺癌合并 ILD 患者。Meta 分析表明,男性[比值比(ORs)=1.78,95%置信区间(CI):1.02-3.11,P=0.041]、CT 上通常为间质性肺炎模式(OR=1.52,95%CI:1.06-2.17,P=0.021)、Krebs von den Lungen-6[标准化均数差(SMD)=0.50,95%CI:0.06-0.94,P=0.027]、白细胞(SMD=0.53,95%CI:0.12-0.93,P=0.010)、乳酸脱氢酶(SMD=0.47,95%CI:0.04-0.90,P=0.032)、氧分压(加权均数差=-3.09,95%CI:-5.99 至-0.19,P=0.037)、手术方式(OR=2.31,95%CI:1.42-3.77,P<0.001)和手术时间(加权均数差=28.26,95%CI:1.13-55.39,P=0.041)是肺癌切除术后 ILD AE 的危险因素。
我们发现男性、CT 上通常为间质性肺炎模式、较高的 Krebs von den Lungen-6、乳酸脱氢酶、白细胞、较低的氧分压、较大的手术范围和较长的手术时间是肺癌切除术后 ILD AE 的危险因素。具有这些危险因素的患者应更慎重地选择手术治疗,并在术后更密切地监测。