MMWR Morb Mortal Wkly Rep. 2022 Jan 21;71(3):96-102. doi: 10.15585/mmwr.mm7103e1.
The COVID-19 pandemic has magnified longstanding health care and social inequities, resulting in disproportionately high COVID-19-associated illness and death among members of racial and ethnic minority groups (1). Equitable use of effective medications (2) could reduce disparities in these severe outcomes (3). Monoclonal antibody (mAb) therapies against SARS-CoV-2, the virus that causes COVID-19, initially received Emergency Use Authorization (EUA) from the Food and Drug Administration (FDA) in November 2020. mAbs are typically administered in an outpatient setting via intravenous infusion or subcutaneous injection and can prevent progression of COVID-19 if given after a positive SARS-CoV-2 test result or for postexposure prophylaxis in patients at high risk for severe illness. Dexamethasone, a commonly used steroid, and remdesivir, an antiviral drug that received EUA from FDA in May 2020, are used in inpatient settings and help prevent COVID-19 progression (2). No large-scale studies have yet examined the use of mAb by race and ethnicity. Using COVID-19 patient electronic health record data from 41 U.S. health care systems that participated in the PCORnet, the National Patient-Centered Clinical Research Network, this study assessed receipt of medications for COVID-19 treatment by race (White, Black, Asian, and Other races [including American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, and multiple or Other races]) and ethnicity (Hispanic or non-Hispanic). Relative disparities in mAb** treatment among all patients (805,276) with a positive SARS-CoV-2 test result and in dexamethasone and remdesivir treatment among inpatients (120,204) with a positive SARS-CoV-2 test result were calculated. Among all patients with positive SARS-CoV-2 test results, the overall use of mAb was infrequent, with mean monthly use at 4% or less for all racial and ethnic groups. Hispanic patients received mAb 58% less often than did non-Hispanic patients, and Black, Asian, or Other race patients received mAb 22%, 48%, and 47% less often, respectively, than did White patients during November 2020-August 2021. Among inpatients, disparities were different and of lesser magnitude: Hispanic inpatients received dexamethasone 6% less often than did non-Hispanic inpatients, and Black inpatients received remdesivir 9% more often than did White inpatients. Vaccines and preventive measures are the best defense against infection; use of COVID-19 medications postexposure or postinfection can reduce morbidity and mortality and relieve strain on hospitals but are not a substitute for COVID-19 vaccination. Public health policies and programs centered around the specific needs of communities can promote health equity (4). Equitable receipt of outpatient treatments, such as mAb and antiviral medications, and implementation of prevention practices are essential to reducing existing racial and ethnic inequities in severe COVID-19-associated illness and death.
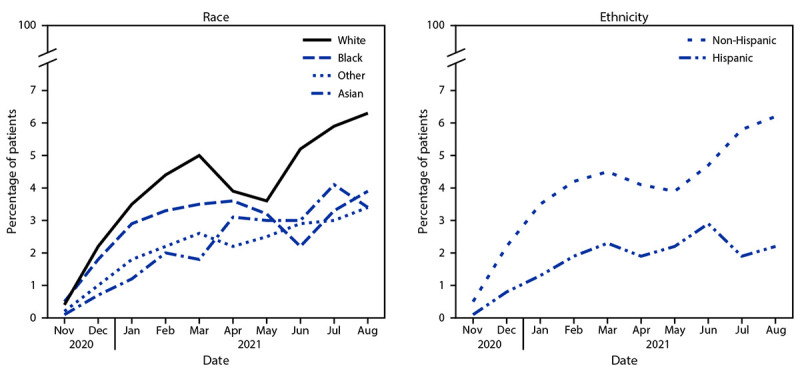
新型冠状病毒肺炎大流行使长期存在的医疗保健和社会不平等问题更加严重,导致少数族裔群体成员 COVID-19 相关疾病和死亡的比例过高(1)。公平使用有效的药物(2)可以减少这些严重后果(3)中的差异。针对导致 COVID-19 的 SARS-CoV-2 病毒的单克隆抗体 (mAb) 疗法于 2020 年 11 月首次获得美国食品和药物管理局 (FDA) 的紧急使用授权 (EUA)。mAb 通常在门诊环境中通过静脉输注或皮下注射给药,如果在 SARS-CoV-2 检测结果呈阳性后给予,或在高风险严重疾病的患者中进行暴露后预防,可预防 COVID-19 的进展(2)。通常使用的类固醇地塞米松和 2020 年 5 月获得 FDA EUA 的抗病毒药物瑞德西韦在住院环境中使用,并有助于预防 COVID-19 的进展(2)。目前还没有大规模研究检查 mAb 按种族和族裔使用的情况。本研究利用来自参与 PCORnet(国家以患者为中心的临床研究网络)的 41 个美国医疗保健系统的 COVID-19 患者电子健康记录数据,评估了按种族(白种人、黑种人、亚洲人和其他种族[包括美洲印第安人或阿拉斯加原住民、夏威夷原住民或其他太平洋岛民以及多种或其他种族])和族裔(西班牙裔或非西班牙裔)接受 COVID-19 治疗药物的情况。计算了所有 SARS-CoV-2 检测呈阳性的患者(805,276 人)中 mAb 治疗的相对差异,以及所有 SARS-CoV-2 检测呈阳性的住院患者(120,204 人)中地塞米松和瑞德西韦治疗的相对差异。在所有 SARS-CoV-2 检测呈阳性的患者中,mAb 的总体使用频率较低,所有种族和族裔群体的平均每月使用率均为 4%或更低。与非西班牙裔患者相比,西班牙裔患者接受 mAb 的频率低 58%,黑种人、亚洲人或其他种族患者接受 mAb 的频率分别低 22%、48%和 47%。2020 年 11 月至 2021 年 8 月期间。在住院患者中,差异不同且程度较小:与非西班牙裔患者相比,西班牙裔住院患者接受地塞米松的频率低 6%,与白人住院患者相比,黑种人住院患者接受瑞德西韦的频率高 9%。疫苗和预防措施是预防感染的最佳方法;暴露后或感染后使用 COVID-19 药物可以降低发病率和死亡率,并减轻医院的压力,但不能替代 COVID-19 疫苗接种。以社区的具体需求为中心的公共卫生政策和计划可以促进健康公平(4)。公平获得门诊治疗,如 mAb 和抗病毒药物,并实施预防措施,对于减少与 COVID-19 相关的严重疾病和死亡的现有种族和族裔不平等至关重要。