Dept. of Medicine, Division of Endocrinology, and Centre for Endocrine Tumors Leiden, Leiden University Medical Center, Leiden, the Netherlands.
Leiden University Medical Center, Haaglanden Medical Center and Haga Teaching Hospitals, University Neurosurgical Center Holland, Leiden and The Hague, the Netherlands.
Endocrine. 2022 Apr;76(1):132-141. doi: 10.1007/s12020-022-02983-3. Epub 2022 Jan 24.
The condition of pituitary apoplexia contains the clinical spectre from life-threatening emergency to asymptomatic self-limiting course, which partly determines diagnostic delay and management. Outcome evaluation of course and management of pituitary apoplexia is hampered by the diverse presentation of this condition and requires appraisal. This study aimed to describe the patient journey, clinical presentation, and management of various types of pituitary apoplexy in a new classification to facilitate future outcome evaluation and identify unmet needs in the care process.
A single-center retrospective patient chart study was conducted between 2005-2021 (N = 98). Outcome measures were clinical symptoms at first presentation in hospital, being headache, consciousness, visual acuity, visual field defects (VFD), ophthalmoplegia, nausea, vomiting, fever, and hypopituitarism and care process characteristics.
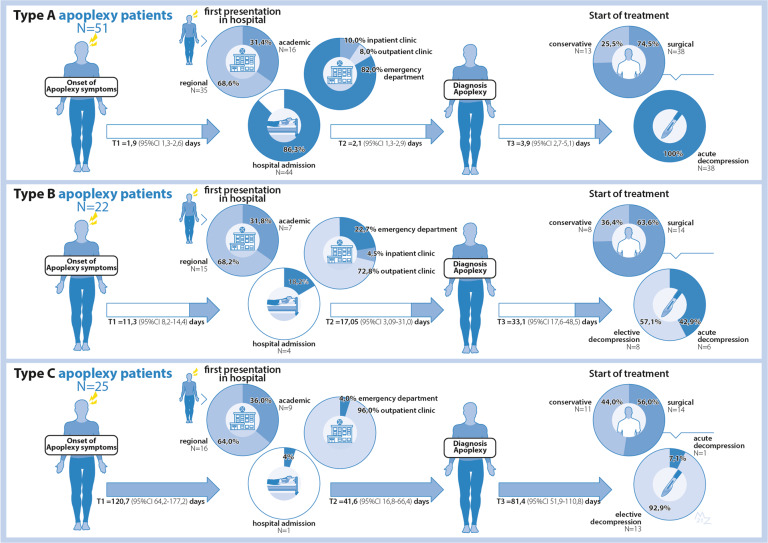
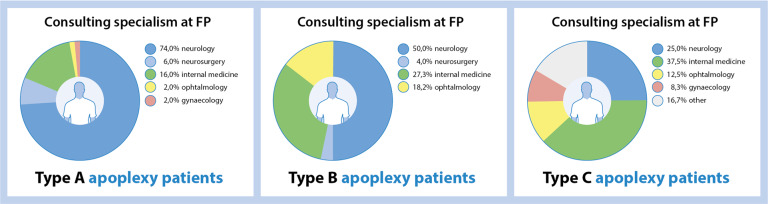
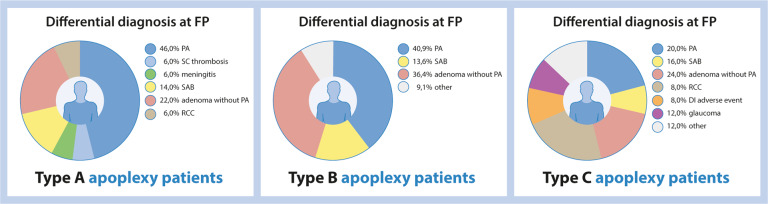
Mean age was 47.6 ± 16.6 years (51.0% male). We describe their patient journey and identified three different types, differing in clinical presentation, in-hospital route, and final treatment, e.g., Acute (type A, 52%), Subacute (type B, 22.5%), and Non-acute (type C, 25.5%). Type A generally presents with acute onset headaches, VFD, or ophthalmoplegia emergency setting, with lowest mean visual acuity of both eyes and frequent hypocortisolism.
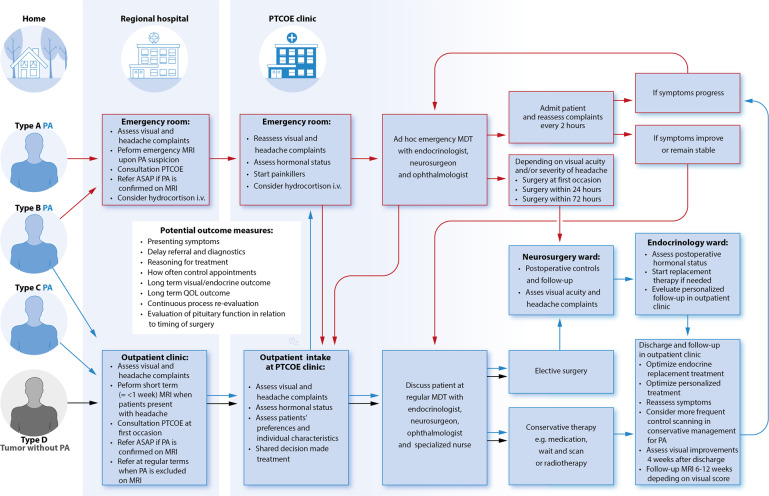
Pituitary apoplexy can be approached as a spectrum of disease with 3 main subtypes, with a different initial presentation, different in-hospital route resulting in different management. Acknowledging subtypes with particular needs for (emergency) referrals to Pituitary Tumors Center of Excellence (PTCOE) will serve patient care improvements, outcome evaluations and address areas for improvement.
垂危性的垂体卒中包含了从危及生命的急症到无症状自限性病程的临床谱,这在一定程度上导致了诊断延迟和管理不当。由于这种情况的表现多种多样,因此对垂体卒中病程和管理的结果评估受到了阻碍,需要进行评估。本研究旨在描述新分类中各种类型的垂体卒中患者的就诊过程、临床表现和管理,以方便对未来结果进行评估,并确定在护理过程中未满足的需求。
对 2005 年至 2021 年期间的 98 例单中心回顾性患者病历进行了研究。主要观察指标为住院时首次出现的临床症状,包括头痛、意识、视力、视野缺损(VFD)、眼肌麻痹、恶心、呕吐、发热和垂体功能减退,以及护理过程的特点。
患者的平均年龄为 47.6±16.6 岁(51.0%为男性)。我们描述了他们的就诊过程,并确定了三种不同的类型,它们在临床表现、住院途径和最终治疗上有所不同,例如急性型(A型,52%)、亚急性型(B 型,22.5%)和非急性型(C 型,25.5%)。A型通常表现为急性头痛、VFD 或眼肌麻痹的急症,双眼视力最低,且皮质醇功能减退症较为常见。
垂体卒中可以作为一种疾病谱来处理,有 3 个主要亚型,其初始表现不同,住院途径不同,导致管理方式不同。认识到具有特殊转诊(紧急转诊)到垂体肿瘤卓越中心(PTCOE)需求的亚型,将有助于改善患者护理、结果评估,并解决需要改进的领域。