Decision Modeling Center, Department of Epidemiology and Data Science, 1209Amsterdam University Medical Center, Amsterdam, The Netherlands.
Department of Public Health, 6993Erasmus University Medical Center, Rotterdam, The Netherlands.
J Med Screen. 2022 Jun;29(2):72-83. doi: 10.1177/09691413211056777. Epub 2021 Dec 3.
Colorectal cancer (CRC) screening with a faecal immunochemical test (FIT) has been disrupted in many countries during the COVID-19 pandemic. Performing catch-up of missed screens while maintaining regular screening services requires additional colonoscopy capacity that may not be available. This study aimed to compare strategies that clear the screening backlog using limited colonoscopy resources.
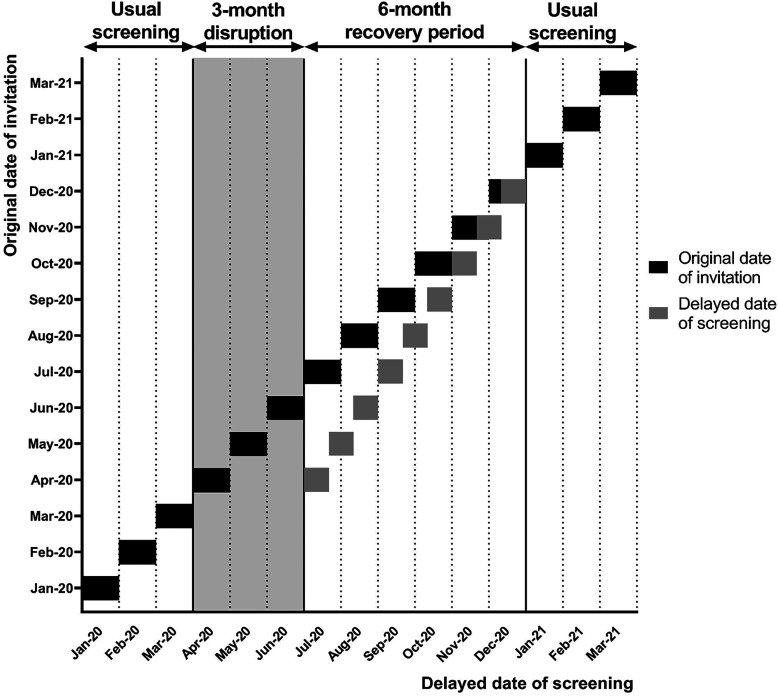
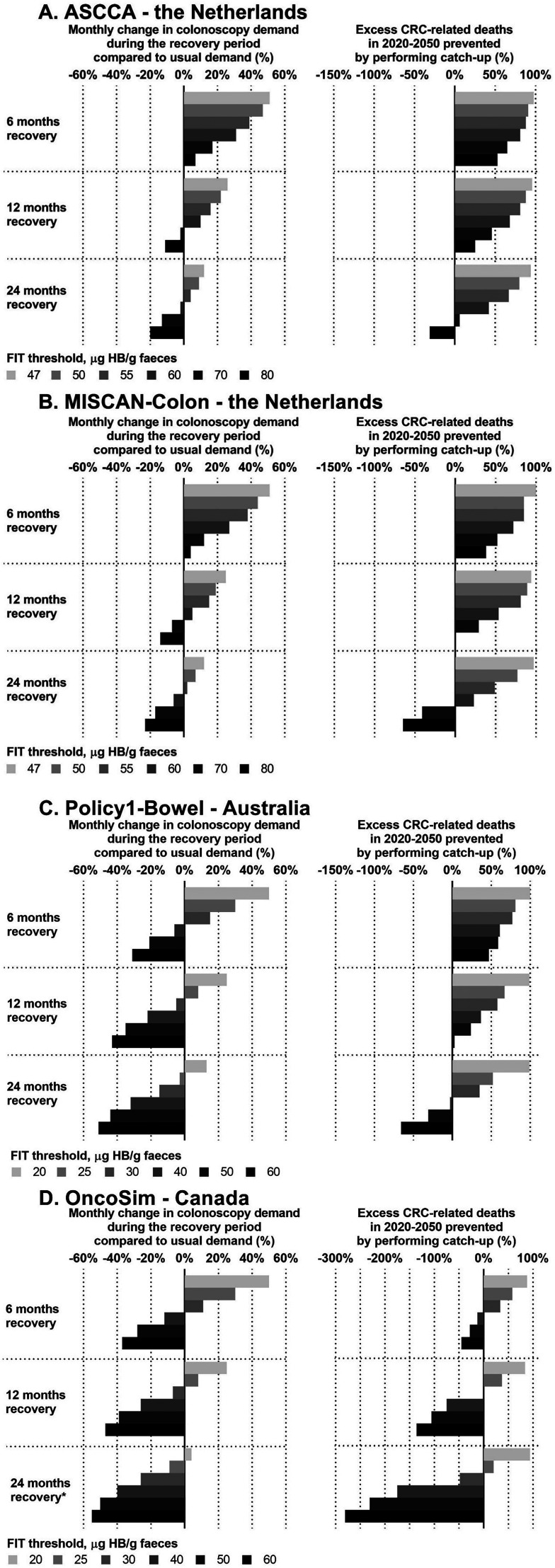
A range of strategies were simulated using four country-specific CRC natural-history models: Adenoma and Serrated pathway to Colorectal CAncer (ASCCA) and MIcrosimulation SCreening ANalysis for CRC (MISCAN-Colon) (both in the Netherlands), Policy1-Bowel (Australia) and OncoSim (Canada). Strategies assumed a 3-month screening disruption with varying recovery period lengths (6, 12, and 24 months) and varying FIT thresholds for diagnostic colonoscopy. Increasing the FIT threshold reduces the number of referrals to diagnostic colonoscopy. Outcomes for each strategy were colonoscopy demand and excess CRC-related deaths due to the disruption.
Performing catch-up using the regular FIT threshold in 6, 12 and 24 months could prevent most excess CRC-related deaths, but required 50%, 25% and 12.5% additional colonoscopy demand, respectively. Without exceeding usual colonoscopy demand, up to 60% of excess CRC-related deaths can be prevented by increasing the FIT threshold for 12 or 24 months. Large increases in FIT threshold could lead to additional deaths rather than preventing them.
Clearing the screening backlog in 24 months could avert most excess CRC-related deaths due to a 3-month disruption but would require a small increase in colonoscopy demand. Increasing the FIT threshold slightly over 24 months could ease the pressure on colonoscopy resources.
在 COVID-19 大流行期间,许多国家的粪便免疫化学检测(FIT)结直肠癌(CRC)筛查工作受到了干扰。在维持常规筛查服务的同时,进行错过筛查的追赶需要额外的结肠镜检查能力,而这些能力可能并不具备。本研究旨在比较使用有限结肠镜资源清除筛查积压的策略。
使用四个特定于国家的 CRC 自然史模型模拟了一系列策略:腺瘤和锯齿状途径至结直肠癌(ASCCA)和微模拟筛查分析结直肠癌(MISCAN-Colon)(均在荷兰)、政策 1-肠道(澳大利亚)和 OncoSim(加拿大)。这些策略假设筛查中断持续 3 个月,恢复期长度不同(6、12 和 24 个月),诊断性结肠镜检查的 FIT 阈值也不同。增加 FIT 阈值会减少转介至诊断性结肠镜检查的人数。每种策略的结果是结肠镜检查需求和因中断而导致的 CRC 相关超额死亡人数。
在 6、12 和 24 个月内使用常规 FIT 阈值进行追赶可以预防大多数 CRC 相关的超额死亡,但分别需要增加 50%、25%和 12.5%的额外结肠镜检查需求。不超过常规结肠镜检查需求,通过增加 FIT 阈值 12 或 24 个月,最多可以预防 60%的 CRC 相关超额死亡。大幅增加 FIT 阈值可能会导致额外的死亡,而不是预防这些死亡。
在 24 个月内清除筛查积压可以避免由于 3 个月的中断而导致的大多数 CRC 相关死亡,但需要增加少量的结肠镜检查需求。将 FIT 阈值略微提高超过 24 个月可能会缓解结肠镜检查资源的压力。