Liver Failure Group, Institute for Liver and Digestive Health, University College London, London, UK.
Faculty of Medicine, Alexandria University, Alexandria, Egypt.
Aliment Pharmacol Ther. 2022 Mar;55(6):722-732. doi: 10.1111/apt.16790. Epub 2022 Feb 1.
The occurrence of overt hepatic encephalopathy (OHE) is associated with increased mortality. HE is commonly precipitated by infection, but whether HE predisposes to new infection is unclear. This study aimed to test if OHE predisposes to de novo infection during hospitalisation and its association with short-term mortality.
Seven hundred and fifty-nine consecutive patients were identified at two institutions from prospectively maintained clinical databases of cirrhotic patients admitted with acute decompensation (AD). Infection and HE data were collected on the day of admission, and the occurrence of de novo infections was assessed for 28 days after admission. EASL-CLIF organ failure criteria were used to determine the presence of organ failures. Multivariable analysis using the logistic regression model was used to assess predictors of 28-day mortality and de novo infection.
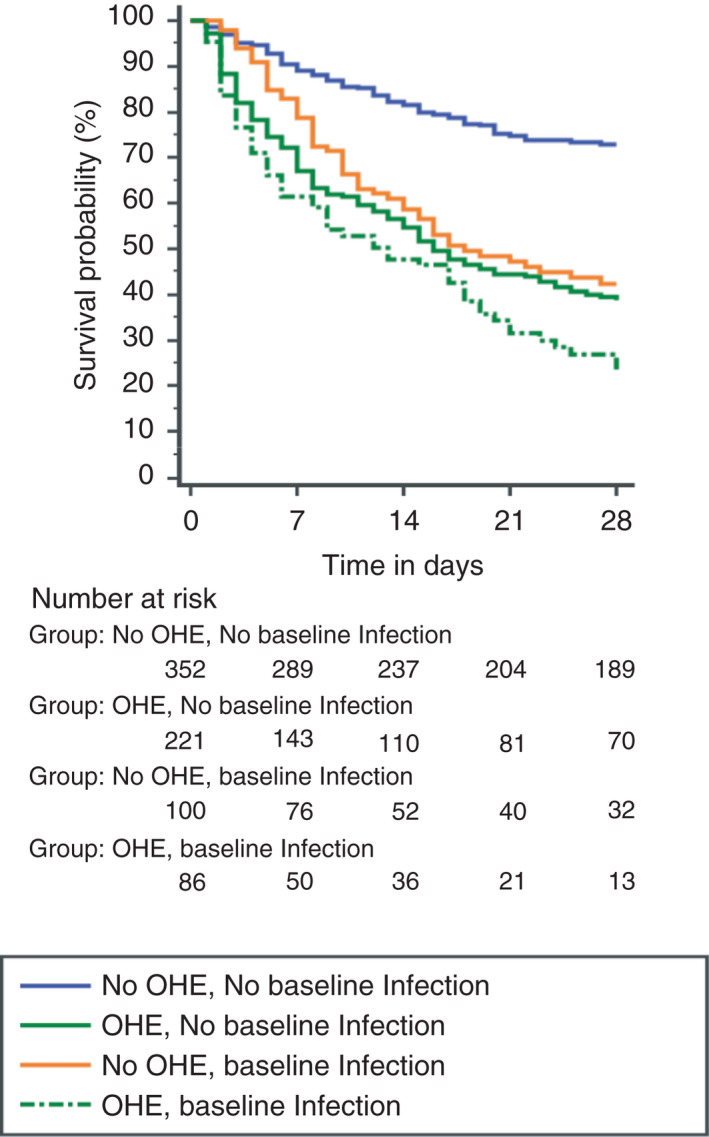
Patients were divided into four groups; no baseline OHE or infection (n = 352); OHE with no baseline Infection (n = 221); no OHE but baseline infection (n = 100) and OHE with baseline infection (n = 86). On multivariate analyses, OHE (OR, 1.532 [95% CI, 1.061-2.300, P = 0.024]), and admission to ITU (OR, 2.303 [95% CI, 1.508-3.517, P < 0.001]) were independent risk factors for de novo infection. 28-day mortality was 25.3%, 60.2%, 55.0% and 72.1% in the 4-groups respectively. Age, INR and creatinine were independently predictive of mortality. The presence of overt HE, infection, coagulation, kidney, circulatory, respiratory and liver failures were significantly associated with higher mortality.
OHE is an independent risk factor for de novo infection in cirrhotic patients with AD.
显性肝性脑病(OHE)的发生与死亡率增加有关。HE 通常由感染引发,但 HE 是否易引发新的感染尚不清楚。本研究旨在检验 OHE 是否易在住院期间引发新的感染及其与短期死亡率的关系。
从两家机构前瞻性维护的肝硬化患者急性失代偿(AD)入院临床数据库中确定了 759 例连续患者。入院当天收集感染和 HE 数据,并在入院后 28 天评估新感染的发生情况。采用 EASL-CLIF 器官衰竭标准确定器官衰竭的存在。采用逻辑回归模型的多变量分析用于评估 28 天死亡率和新发感染的预测因素。
患者分为四组:无基线 OHE 或感染(n=352);无基线感染但有 OHE(n=221);无 OHE 但有基线感染(n=100)和有基线感染且有 OHE(n=86)。多变量分析显示,OHE(OR,1.532 [95%CI,1.061-2.300,P=0.024])和 ICU 入院(OR,2.303 [95%CI,1.508-3.517,P<0.001])是新发感染的独立危险因素。四组的 28 天死亡率分别为 25.3%、60.2%、55.0%和 72.1%。年龄、INR 和肌酐是死亡率的独立预测因素。显性 HE、感染、凝血、肾脏、循环、呼吸和肝脏衰竭的存在与更高的死亡率显著相关。
OHE 是肝硬化 AD 患者新发感染的独立危险因素。