Human Oncology and Pathogenesis Program, Memorial Sloan Kettering Cancer Center, New York, New York.
Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York.
Clin Cancer Res. 2022 Apr 14;28(8):1507-1517. doi: 10.1158/1078-0432.CCR-21-3909.
This phase Ib trial was designed to evaluate the safety and early efficacy signal of the combination of imatinib and binimetinib in patients with imatinib-resistant advanced gastrointestinal stromal tumors (GISTs).
This trial used a standard 3 + 3 design to determine the recommended phase II dose (RP2D). Additional patients were enrolled on an expansion cohort at the RP2D enriching for succinate dehydrogenase (SDH)-deficient GISTs to explore potential efficacy.
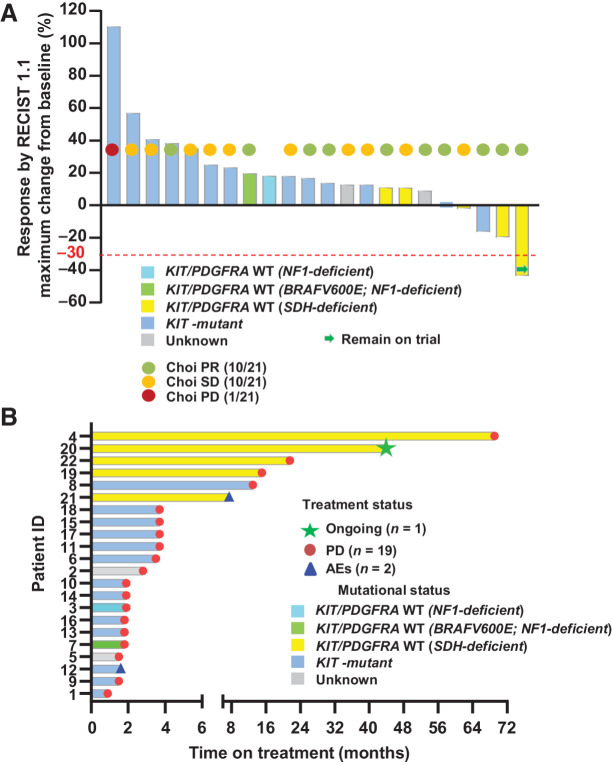
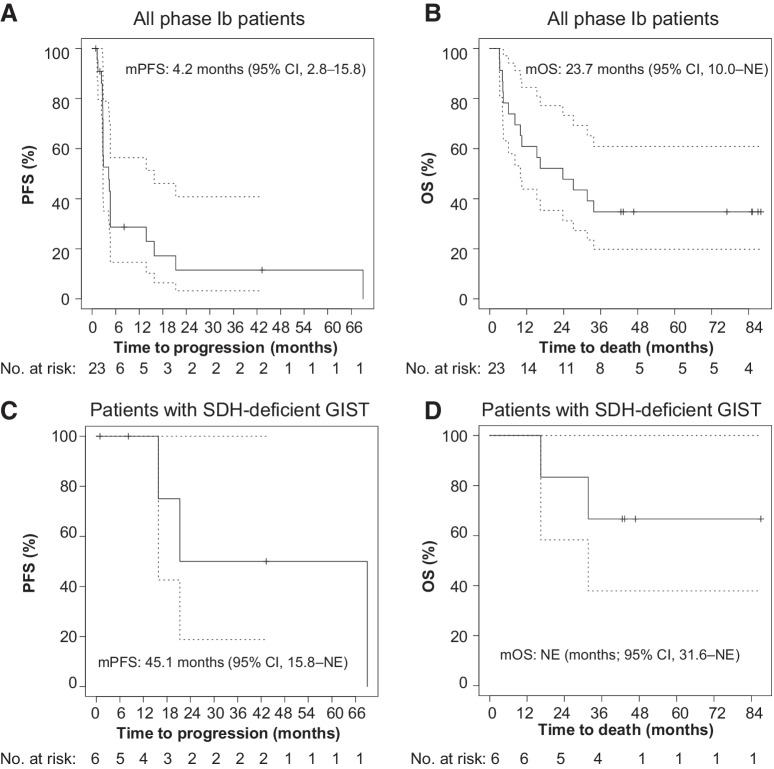
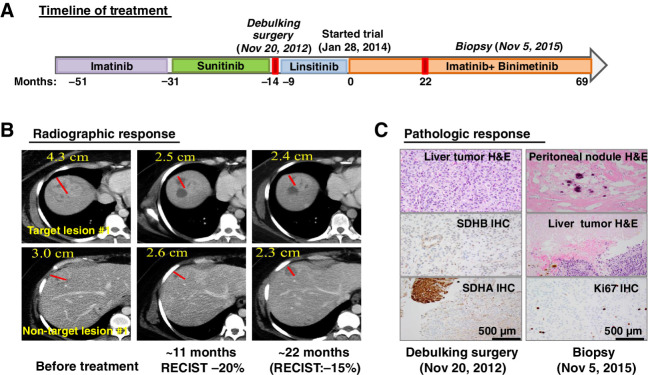
The trial enrolled nine patients in the dose-escalation cohort and 14 in the dose-expansion cohort including six with SDH-deficient GISTs. Imatinib 400 mg daily with binimetinib 45 mg twice daily was established as the RP2D. Dose-limiting toxicity (DLT) was asymptomatic grade 4 creatinine phosphokinase (CPK) elevation. The most common non-DLT grade 3/4 toxicity was asymptomatic CPK elevation (69.6%). Other common ≥grade 2 toxicities included peripheral edema (17.4%), acneiform rash (21.7%), anemia (30.4%), hypophosphatemia (39.1%), and aspartate aminotransferase (AST) increase (17.4%). Two serious adverse events occurred (grade 2 dropped head syndrome and grade 3 central retinal vein occlusion). No unexpected toxicities were observed. Limited clinical activity was observed in KIT-mutant GIST. For SDH-deficient GISTs, one of five had confirmed RECIST1.1 partial response (PR). The median progression-free survival (mPFS) in patients with SDH-deficient GIST was 45.1 months [95% confidence interval (CI), 15.8-not estimable (NE)]; the median overall survival (mOS) was not reached (95% CI, 31.6 months-NE). One patient with a refractory metastatic SDH-deficient GIST had an exceptional pathologic response and durable clinical benefit.
The combination of imatinib and binimetinib is safe with manageable toxicity and has encouraging activity in SDH-deficient but not imatinib-refractory KIT/PDGFRA-mutant GISTs. The observed clinical benefits provide a motivation for a larger trial of the combination strategy in SDH-deficient GISTs.
本Ib 期试验旨在评估伊马替尼联合 binimetinib 治疗伊马替尼耐药的晚期胃肠道间质瘤(GIST)患者的安全性和早期疗效信号。
本试验采用标准的 3+3 设计来确定推荐的 II 期剂量(RP2D)。在 RP2D 时,在扩展队列中招募更多的患者,富集琥珀酸脱氢酶(SDH)缺陷的 GIST,以探索潜在的疗效。
试验纳入了剂量递增队列的 9 名患者和剂量扩展队列的 14 名患者,其中 6 名患者患有 SDH 缺陷的 GIST。每日 400mg 伊马替尼联合每日两次 45mg binimetinib 被确定为 RP2D。剂量限制毒性(DLT)为无症状的 4 级肌酸磷酸激酶(CPK)升高。最常见的非 DLT 3/4 级毒性为无症状的 CPK 升高(69.6%)。其他常见的≥2 级毒性包括外周水肿(17.4%)、痤疮样皮疹(21.7%)、贫血(30.4%)、低磷血症(39.1%)和天门冬氨酸氨基转移酶(AST)升高(17.4%)。发生了 2 起严重不良事件(2 级垂头综合征和 3 级视网膜中央静脉阻塞)。未观察到意外毒性。在 KIT 突变的 GIST 中观察到有限的临床活性。对于 SDH 缺陷的 GIST,5 例中有 1 例确认 RECIST1.1 部分缓解(PR)。SDH 缺陷 GIST 患者的中位无进展生存期(mPFS)为 45.1 个月[95%置信区间(CI),15.8-不可估计(NE)];中位总生存期(mOS)未达到(95%CI,31.6 个月-NE)。1 例难治性转移性 SDH 缺陷 GIST 患者出现了异常的病理性反应和持久的临床获益。
伊马替尼联合 binimetinib 联合治疗安全,毒性可管理,在 SDH 缺陷但不是伊马替尼耐药的 KIT/PDGFRA 突变的 GIST 中具有令人鼓舞的疗效。观察到的临床获益为在 SDH 缺陷的 GIST 中进行更大规模的联合治疗策略试验提供了动力。