Université de Paris, Paris, France.
Département de Gynécologie Obstétrique II et Médecine de la Reproduction, Assistance Publique-Hôpitaux de Paris (AP-HP), Centre Hospitalier Universitaire (CHU) Cochin, Hôpital Universitaire Paris Centre (HUPC), Paris, France.
JAMA Netw Open. 2022 Feb 1;5(2):e2147788. doi: 10.1001/jamanetworkopen.2021.47788.
Endometriosis is an inflammatory disease with a heterogeneous presentation that affects women of childbearing age. Given the limitations of previous retrospective studies, it is still unclear whether endometriosis has adverse implications for pregnancy outcomes.
To evaluate the association between the presence of endometriosis and preterm birth and whether the risk varied according to the disease phenotype.
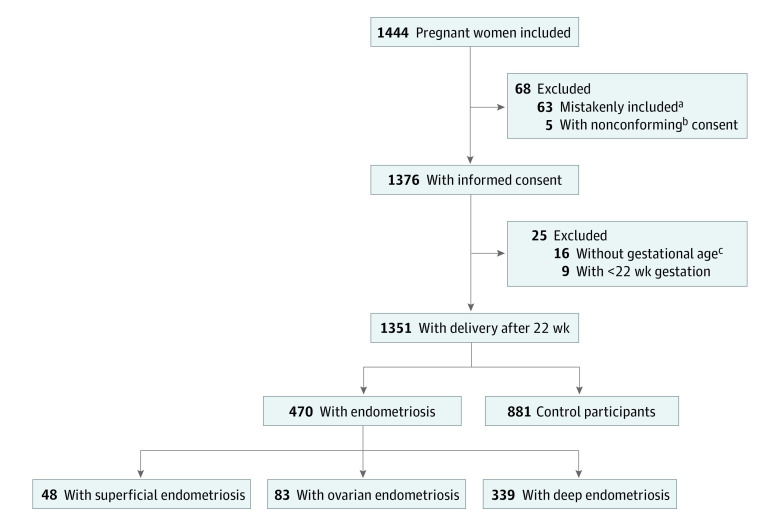
DESIGN, SETTING, AND PARTICIPANTS: This cohort study with exposed and unexposed groups was conducted in 7 maternity units in France from February 4, 2016, to June 28, 2018. Participants included women with singleton pregnancies who were followed up before 22 weeks' gestation along with their newborns delivered at or after 22 weeks' gestation. The final follow-up occurred in July 2019. Data were analyzed from October 7, 2020, to February 7, 2021.
Women in the endometriosis group had a documented history of endometriosis and were classified according to 3 endometriosis phenotypes: isolated superficial peritoneal endometriosis (SUP), ovarian endometrioma (OMA; potentially associated with SUP), and deep endometriosis (DE; potentially associated with SUP and OMA). Women in the control group did not have a history of clinical symptoms of endometriosis before their current pregnancy.
The primary outcome was preterm birth between 22 weeks and 36 weeks 6 days of gestation. Association between endometriosis and the primary outcome was assessed through univariate and multivariate logistic regression analyses and was adjusted for the following risk factors associated with preterm birth: maternal age, body mass index (calculated as weight in kilograms divided by height in meters squared) before pregnancy, country of birth, parity, previous cesarean delivery, history of myomectomy and hysteroscopy, and preterm birth. The same analysis was performed according to the 3 endometriosis phenotypes (SUP, OMA, and DE).
Of the 1351 study participants (mean [SD] age, 32.9 [5.0] years) who had a singleton delivery after 22 weeks of gestation, 470 were assigned to the endometriosis group (48 had SUP [10.2%], 83 had OMA [17.7%], and 339 had DE [72.1%]) and 881 were assigned to the control group. No difference was observed in the rate of preterm deliveries before 37 weeks 0 days of gestation between the endometriosis and control groups (34 of 470 [7.2%] vs 53 of 881 [6.0%]; P = .38). After adjusting for confounding factors, endometriosis was not associated with preterm birth before 37 weeks' gestation (adjusted odds ratio, 1.07; 95% CI, 0.64-1.77). The results were comparable for the different disease phenotypes (SUP: 6.2% [3 of 48]; OMA: 7.2% [6 of 83]; and DE: 7.4% [25 of 339]; P = .84).
This cohort study found no association between endometriosis and preterm birth, and the disease phenotype did not appear to alter the result. Monitoring the pregnancy beyond the normal protocols or changing management strategies for women with endometriosis may not be warranted to prevent preterm birth.
子宫内膜异位症是一种具有异质表现的炎症性疾病,影响育龄妇女。鉴于以前回顾性研究的局限性,子宫内膜异位症是否对妊娠结局有不良影响仍不清楚。
评估子宫内膜异位症与早产之间的关联,以及这种风险是否因疾病表型而异。
设计、地点和参与者:这项队列研究设有暴露组和非暴露组,在法国的 7 家产科单位进行,时间为 2016 年 2 月 4 日至 2018 年 6 月 28 日。参与者包括在 22 周妊娠前接受随访的单胎妊娠妇女,以及在 22 周或 22 周后分娩的新生儿。最终随访发生在 2019 年 7 月。数据分析于 2020 年 10 月 7 日至 2021 年 2 月 7 日进行。
子宫内膜异位症组的女性有子宫内膜异位症病史,并根据 3 种子宫内膜异位症表型进行分类:单纯性腹膜内子宫内膜异位症(SUP)、卵巢子宫内膜瘤(OMA;可能与 SUP 相关)和深部子宫内膜异位症(DE;可能与 SUP 和 OMA 相关)。对照组的女性在当前妊娠前没有子宫内膜异位症的临床症状史。
主要结局是 22 周至 36 周 6 天之间的早产。通过单变量和多变量逻辑回归分析评估子宫内膜异位症与主要结局之间的关联,并根据与早产相关的以下风险因素进行调整:母亲年龄、妊娠前体重指数(体重以千克为单位,身高以米为单位)、出生国、产次、既往剖宫产、子宫肌瘤切除术和宫腔镜检查史,以及早产。根据 3 种子宫内膜异位症表型(SUP、OMA 和 DE)进行了相同的分析。
在 1351 名接受 22 周后分娩的单胎妊娠研究参与者中(平均[SD]年龄,32.9[5.0]岁),470 名参与者被分配到子宫内膜异位症组(48 名患有 SUP[10.2%],83 名患有 OMA[17.7%],339 名患有 DE[72.1%]),881 名参与者被分配到对照组。子宫内膜异位症组和对照组在 37 周 0 天前早产的发生率无差异(子宫内膜异位症组 34/470[7.2%] vs 对照组 53/881[6.0%];P=0.38)。在调整混杂因素后,子宫内膜异位症与 37 周前早产无关(调整后的优势比,1.07;95%CI,0.64-1.77)。不同疾病表型的结果相似(SUP:6.2%[3/48];OMA:7.2%[6/83];DE:7.4%[25/339];P=0.84)。
这项队列研究发现,子宫内膜异位症与早产之间没有关联,疾病表型似乎也没有改变这一结果。对患有子宫内膜异位症的女性进行超出正常方案的妊娠监测或改变管理策略可能没有必要,以预防早产。