Department of Electrophysiology and Cardiac Stimulation, Centre Hospitalier Universitaire de Bordeaux, Bordeaux, France.
Institut Hospitalo-Universitaire Liryc, Electrophysiology and Heart Modeling Institute, Pessac, France.
Eur Heart J. 2022 Mar 21;43(12):1234-1247. doi: 10.1093/eurheartj/ehab893.
Mapping data of human ventricular fibrillation (VF) are limited. We performed detailed mapping of the activities underlying the onset of VF and targeted ablation in patients with structural cardiac abnormalities.
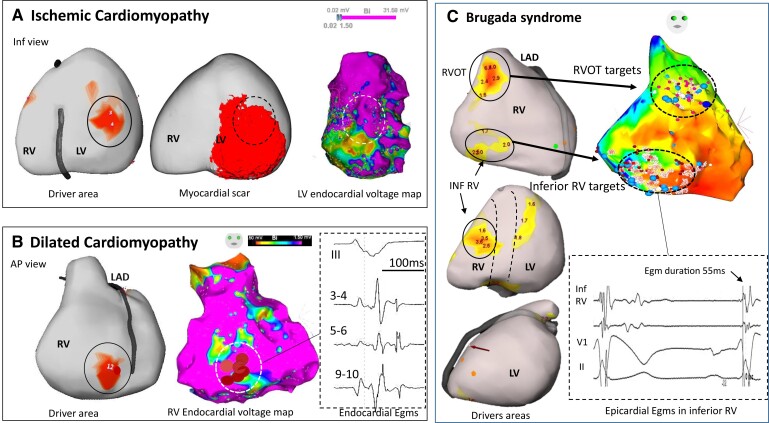
We evaluated 54 patients (50 ± 16 years) with VF in the setting of ischaemic (n = 15), hypertrophic (n = 8) or dilated cardiomyopathy (n = 12), or Brugada syndrome (n = 19). Ventricular fibrillation was mapped using body-surface mapping to identify driver (reentrant and focal) areas and invasive Purkinje mapping. Purkinje drivers were defined as Purkinje activities faster than the local ventricular rate. Structural substrate was delineated by electrogram criteria and by imaging. Catheter ablation was performed in 41 patients with recurrent VF. Sixty-one episodes of spontaneous (n = 10) or induced (n = 51) VF were mapped. Ventricular fibrillation was organized for the initial 5.0 ± 3.4 s, exhibiting large wavefronts with similar cycle lengths (CLs) across both ventricles (197 ± 23 vs. 196 ± 22 ms, P = 0.9). Most drivers (81%) originated from areas associated with the structural substrate. The Purkinje system was implicated as a trigger or driver in 43% of patients with cardiomyopathy. The transition to disorganized VF was associated with the acceleration of initial reentrant activities (CL shortening from 187 ± 17 to 175 ± 20 ms, P < 0.001), then spatial dissemination of drivers. Purkinje and substrate ablation resulted in the reduction of VF recurrences from a pre-procedural median of seven episodes [interquartile range (IQR) 4-16] to 0 episode (IQR 0-2) (P < 0.001) at 56 ± 30 months.
The onset of human VF is sustained by activities originating from Purkinje and structural substrate, before spreading throughout the ventricles to establish disorganized VF. Targeted ablation results in effective reduction of VF burden.
The initial phase of human ventricular fibrillation (VF) is critical as it involves the primary activities leading to sustained VF and arrhythmic sudden death. The origin of such activities is unknown.
Body-surface mapping shows that most drivers (≈80%) during the initial VF phase originate from electrophysiologically defined structural substrates. Repetitive Purkinje activities can be elicited by programmed stimulation and are implicated as drivers in 37% of cardiomyopathy patients.
TAKE-HOME MESSAGE: The onset of human VF is mostly associated with activities from the Purkinje network and structural substrate, before spreading throughout the ventricles to establish sustained VF. Targeted ablation reduces or eliminates VF recurrence.
人类心室颤动(VF)的数据图有限。我们对伴有结构性心脏异常的患者的 VF 发作的起始和靶向消融进行了详细的映射。
我们评估了 54 名 VF 患者(50±16 岁),其中缺血性(n=15)、肥厚性(n=8)或扩张型心肌病(n=12)或 Brugada 综合征(n=19)。使用体表标测确定驱动区(折返和局灶性),采用心外膜标测和侵入性浦肯野纤维标测来确定浦肯野纤维驱动区。浦肯野纤维驱动区定义为比局部心室率快的浦肯野纤维活动。采用电描记图标准和影像学来确定结构性基质。在 41 名复发性 VF 患者中进行了导管消融。对 61 次自发性(n=10)或诱发性(n=51)VF 发作进行了标测。VF 的初始持续时间为 5.0±3.4s,表现为具有相似的周期长度(CL)的大波前,左右心室均相似(197±23 与 196±22ms,P=0.9)。大多数驱动区(81%)起源于与结构性基质相关的区域。浦肯野系统在 43%的心肌病患者中被认为是触发或驱动因素。从最初的折返活动加速(CL 从 187±17 缩短至 175±20ms,P<0.001)到随后的驱动区空间传播,与无序 VF 的发生相关。浦肯野纤维和基质消融使 VF 复发从术前中位数的 7 次(IQR 4-16)减少至 0 次(IQR 0-2)(P<0.001),随访 56±30 个月。
人类 VF 的起始由源自浦肯野纤维和结构性基质的活动维持,然后在整个心室传播,以建立无序的 VF。靶向消融可有效减少 VF 负荷。
人类心室颤动(VF)的初始阶段至关重要,因为它涉及导致持续性 VF 和心律失常性猝死的主要活动。这些活动的起源尚不清楚。
体表标测显示,VF 初始阶段的大多数驱动区(≈80%)起源于电生理学定义的结构性基质。程控刺激可诱发重复性浦肯野纤维活动,并在 37%的心肌病患者中被认为是驱动因素。
人类 VF 的起始主要与浦肯野纤维网络和结构性基质相关的活动有关,然后在整个心室传播,以建立持续性 VF。靶向消融可减少或消除 VF 复发。