Chemical Pathology Unit, Department of Pathology, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia.
Gastroenterology and Hepatology Unit, Department of Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia.
Singapore Med J. 2023 Mar;64(3):188-195. doi: 10.11622/smedj.2022019. Epub 2022 Feb 10.
The diagnosis of Wilson disease (WD) is plagued by biochemical and clinical uncertainties. Thus, calculated parameters have been proposed. This study aimed to: (a) compare the diagnostic values of non-caeruloplasmin copper (NCC), NCC percentage (NCC%), copper-caeruloplasmin ratio (CCR) and adjusted copper in WD; and (b) derive and evaluate a discriminant function in diagnosing WD.
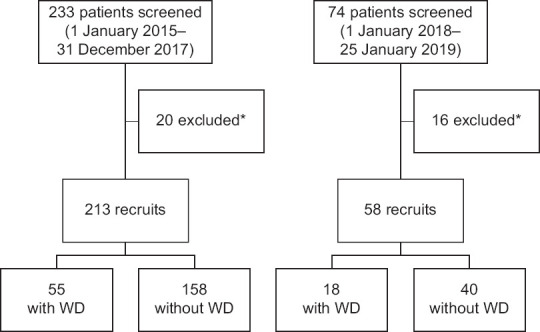
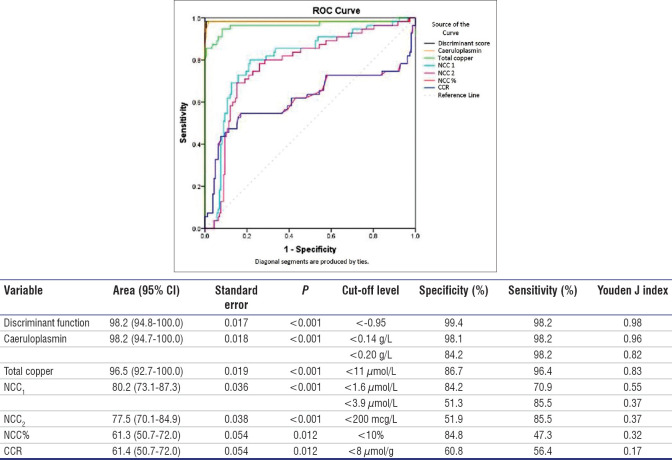
A total of 213 subjects across all ages who were investigated for WD were recruited. WD was confirmed in 55 patients, and the rest were WD free. Based on serum copper and caeruloplasmin values, NCC, NCC%, CCR and adjusted copper were calculated for each subject. A function was derived using discriminant analysis, and the cut-off value was determined through receiver operating characteristic analysis. Classification accuracy was found by cross-tabulation.
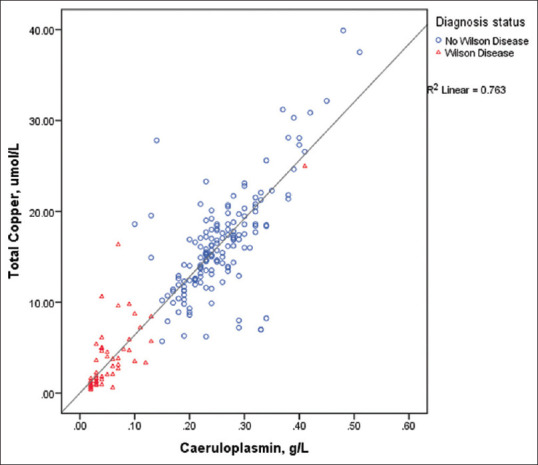
Caeruloplasmin, total copper, NCC, NCC%, CCR, adjusted copper and discriminant function were significantly lower in WD compared to non-WD. Discriminant function showed the best diagnostic specificity (99.4%), sensitivity (98.2%) and classification accuracy (99.1%). Caeruloplasmin levels <0.14 g/L showed higher accuracy than the recommended 0.20 g/L cut-off value (97.7% vs. 87.8%). Similarly, molar NCC below the European cut-off of 1.6 umol/L showed higher accuracy than the American cut-off of 3.9 umol/L (80.3% vs. 59.6%) (P < 0.001). NCC%, mass NCC, CCR and adjusted copper showed poorer performances.
Discriminant function differentiates WD from non-WD with excellent specificity, sensitivity and accuracy. Performance of serum caeruloplasmin <0.14 g/L was better than that of <0.20 g/L. NCC, NCC%, CCR and adjusted copper are not helpful in diagnosing WD.
威尔逊病(WD)的诊断受到生化和临床不确定性的困扰。因此,已经提出了一些计算参数。本研究旨在:(a)比较非铜蓝蛋白铜(NCC)、NCC 百分比(NCC%)、铜-铜蓝蛋白比值(CCR)和调整后的铜在 WD 中的诊断价值;(b)推导并评估诊断 WD 的判别函数。
共招募了 213 名年龄各异的 WD 研究对象。55 例患者确诊为 WD,其余为 WD 阴性。根据血清铜和铜蓝蛋白值,计算每位患者的 NCC、NCC%、CCR 和调整后的铜。使用判别分析推导函数,并通过接收者操作特征分析确定截断值。通过交叉制表确定分类准确性。
与非 WD 相比,WD 患者的铜蓝蛋白、总铜、NCC、NCC%、CCR、调整后的铜和判别函数明显较低。判别函数的诊断特异性(99.4%)、敏感性(98.2%)和分类准确性(99.1%)最高。铜蓝蛋白水平<0.14 g/L 的准确性高于推荐的 0.20 g/L 截断值(97.7%比 87.8%)。同样,摩尔 NCC 低于欧洲截断值 1.6 umol/L 的准确性高于美国截断值 3.9 umol/L(80.3%比 59.6%)(P<0.001)。NCC%、质量 NCC、CCR 和调整后的铜的性能较差。
判别函数可以很好地区分 WD 和非 WD,具有极好的特异性、敏感性和准确性。血清铜蓝蛋白<0.14 g/L 的性能优于<0.20 g/L。NCC、NCC%、CCR 和调整后的铜无助于诊断 WD。