Department of Cardiology, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, 200092, China.
BMC Cardiovasc Disord. 2022 Feb 11;22(1):38. doi: 10.1186/s12872-022-02483-2.
Left atrial appendage closure (LAAC) combined with radiofrequency catheter ablation (RFCA) as a hybrid procedure is commonly performed to treat atrial fibrillation (AF). Although this treatment carries a low risk of coronary artery spasm (CAS), and has never been observed in LAAC procedure, caution still needed to be taken. We presented a case of CAS that occurred in an AF patient during the hybrid procedure.
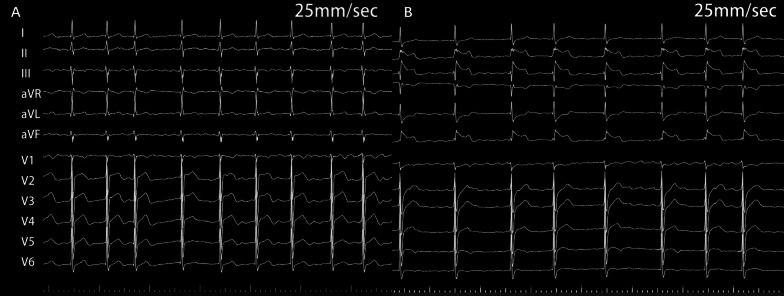
The patient was a 65-year-old man with paroxysmal AF who developed CAS during RFCA and LAAC. In this case, LAAC was performed ahead of RFCA. After atrial septal puncture, the occluder was advanced into left atrium through delivery sheath, and successfully deployed in the LAA. After verifying the assessment of "PASS" criteria, we decided to release the device. However, before releasing the occluder in LAAC, the patient's blood pressure (BP) fell to 70/45 mmHg with heart rate (HR) drop and ST-segment elevation in II, III, and aVF and reciprocal ST-segment depression in I and aVL. Isotonic sodium chloride load was administered. After 3 min, the BP and HR raised, and ST-segment returned to normal. The occluder was successfully released after the stable condition of the patient. Then, RFCA was sequentially performed. When isolating the right pulmonary veins, the patient's BP and HR fell again with ST-segment elevation in inferior leads. Spontaneous ventricular tachycardia and fibrillation developed rapidly and defibrillation was performed immediately with success. Coronary angiography revealed the obstruction of the right coronary artery which disappeared completely after intracoronary nitroglycerin injection (1 mg). Under systemic diltiazem infusion, the RFCA procedure was accomplished. After the procedure, the patient recovered without any neurologic deficit, and CAS has never recurred with isosorbide mononitrate treatment during follow-up.
CAS is a rare complication associated with AF hybrid procedure. Attention should be paid to this rare but potentially life-threatening complication.
左心耳封堵(LAAC)联合射频导管消融(RFCA)作为一种杂交手术,常用于治疗心房颤动(AF)。尽管这种治疗方法发生冠状动脉痉挛(CAS)的风险较低,而且在 LAAC 手术中从未观察到,但仍需谨慎。我们报告了一例在 AF 患者杂交手术中发生的 CAS 病例。
患者为 65 岁阵发性 AF 男性,在 RFCA 和 LAAC 过程中发生 CAS。在这种情况下,LAAC 先于 RFCA 进行。经房间隔穿刺后,输送鞘将封堵器推进左心房,并成功部署在左心耳。在验证“PASS”标准的评估后,我们决定释放设备。然而,在 LAAC 释放封堵器之前,患者的血压(BP)降至 70/45mmHg,心率(HR)下降,II、III 和 aVF 导联 ST 段抬高,I 和 aVL 导联 ST 段对应性压低。给予等渗氯化钠负荷。3 分钟后,BP 和 HR 升高,ST 段恢复正常。患者情况稳定后成功释放封堵器。然后,依次进行 RFCA。当隔离右肺静脉时,患者的 BP 和 HR 再次下降,下壁导联 ST 段抬高。自发性室性心动过速和颤动迅速发展,立即进行电复律并成功。冠状动脉造影显示右冠状动脉阻塞,经冠状动脉内硝酸甘油注射(1mg)后完全消失。在全身地尔硫卓输注下,RFCA 手术完成。手术后,患者恢复良好,无任何神经功能缺损,在随访期间,使用单硝酸异山梨酯治疗后,CAS 从未再发。
CAS 是一种与 AF 杂交手术相关的罕见并发症。应注意这种罕见但可能危及生命的并发症。