Lancet. 2022 Feb 12;399(10325):665-676. doi: 10.1016/S0140-6736(22)00163-5.
Casirivimab and imdevimab are non-competing monoclonal antibodies that bind to two different sites on the receptor binding domain of the SARS-CoV-2 spike glycoprotein, blocking viral entry into host cells. We aimed to evaluate the efficacy and safety of casirivimab and imdevimab administered in combination in patients admitted to hospital with COVID-19.
RECOVERY is a randomised, controlled, open-label platform trial comparing several possible treatments with usual care in patients admitted to hospital with COVID-19. 127 UK hospitals took part in the evaluation of casirivimab and imdevimab. Eligible participants were any patients aged at least 12 years admitted to hospital with clinically suspected or laboratory-confirmed SARS-CoV-2 infection. Participants were randomly assigned (1:1) to either usual standard of care alone or usual care plus casirivimab 4 g and imdevimab 4 g administered together in a single intravenous infusion. Investigators and data assessors were masked to analyses of the outcome data during the trial. The primary outcome was 28-day all-cause mortality assessed by intention to treat, first only in patients without detectable antibodies to SARS-CoV-2 infection at randomisation (ie, those who were seronegative) and then in the overall population. Safety was assessed in all participants who received casirivimab and imdevimab. The trial is registered with ISRCTN (50189673) and ClinicalTrials.gov (NCT04381936).
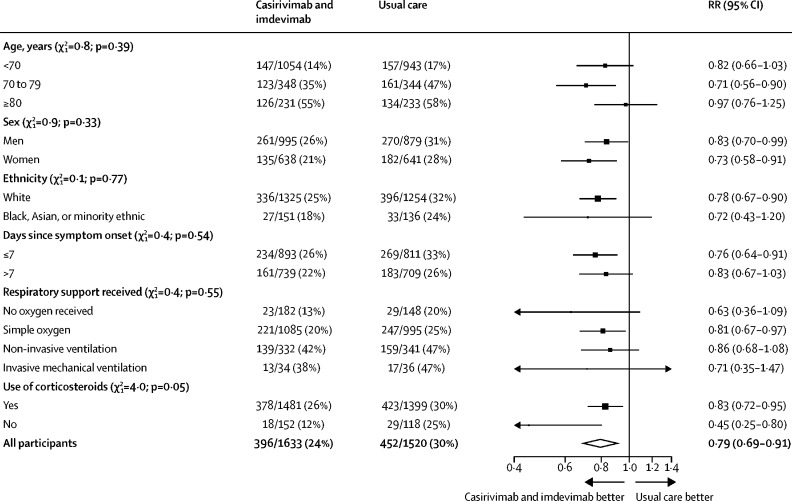
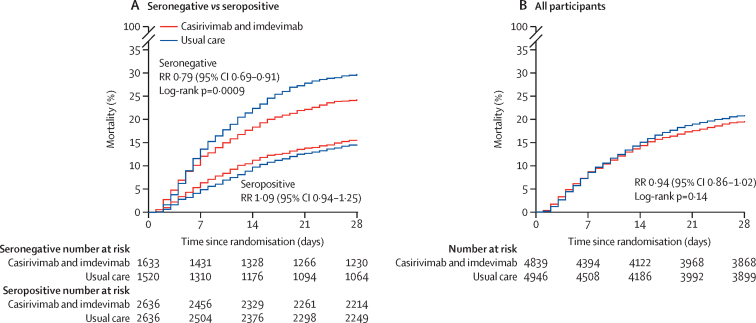
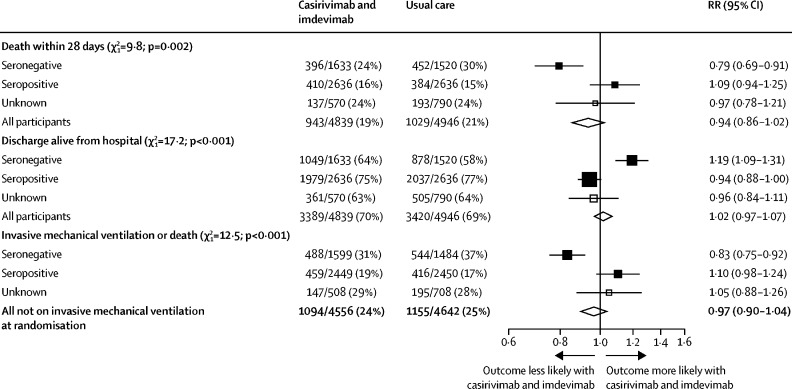
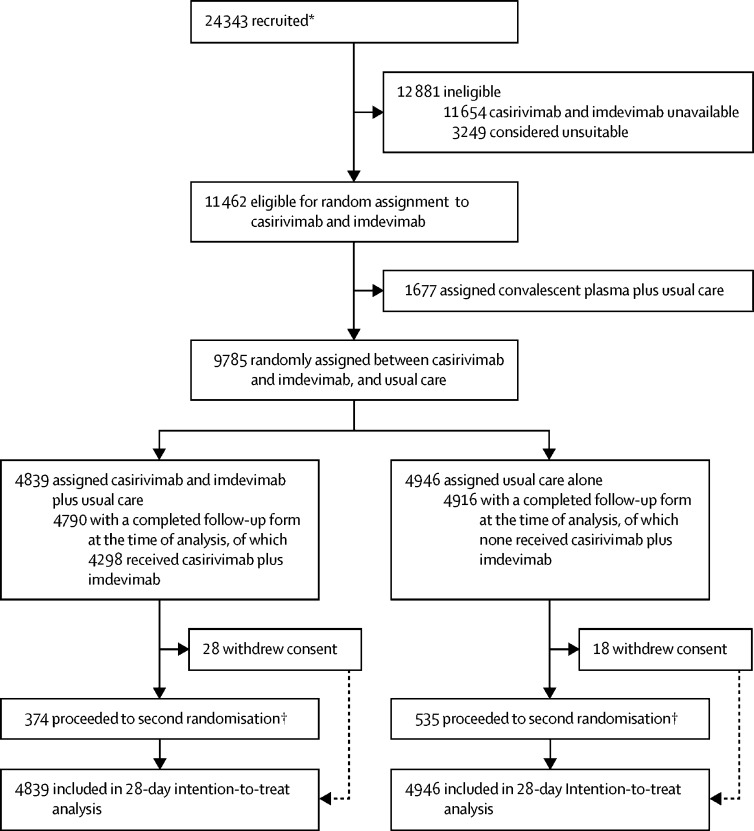
Between Sept 18, 2020, and May 22, 2021, 9785 patients enrolled in RECOVERY were eligible for casirivimab and imdevimab, of which 4839 were randomly assigned to casirivimab and imdevimab plus usual care and 4946 to usual care alone. 3153 (32%) of 9785 patients were seronegative, 5272 (54%) were seropositive, and 1360 (14%) had unknown baseline antibody status. 812 (8%) patients were known to have received at least one dose of a SARS-CoV-2 vaccine. In the primary efficacy population of seronegative patients, 396 (24%) of 1633 patients allocated to casirivimab and imdevimab versus 452 (30%) of 1520 patients allocated to usual care died within 28 days (rate ratio [RR] 0·79, 95% CI 0·69-0·91; p=0·0009). In an analysis of all randomly assigned patients (regardless of baseline antibody status), 943 (19%) of 4839 patients allocated to casirivimab and imdevimab versus 1029 (21%) of 4946 patients allocated to usual care died within 28 days (RR 0·94, 95% CI 0·86-1·02; p=0·14). The proportional effect of casirivimab and imdevimab on mortality differed significantly between seropositive and seronegative patients (p value for heterogeneity=0·002). There were no deaths attributed to the treatment, or meaningful between-group differences in the pre-specified safety outcomes of cause-specific mortality, cardiac arrhythmia, thrombosis, or major bleeding events. Serious adverse reactions reported in seven (<1%) participants were believed by the local investigator to be related to treatment with casirivimab and imdevimab.
In patients admitted to hospital with COVID-19, the monoclonal antibody combination of casirivimab and imdevimab reduced 28-day mortality in patients who were seronegative (and therefore had not mounted their own humoral immune response) at baseline but not in those who were seropositive at baseline.
UK Research and Innovation (Medical Research Council) and National Institute of Health Research.
Casirivimab 和 imdevimab 是两种非竞争的单克隆抗体,它们结合在 SARS-CoV-2 刺突糖蛋白受体结合域的两个不同位点,阻止病毒进入宿主细胞。我们旨在评估 casirivimab 和 imdevimab 联合用于 COVID-19 住院患者的疗效和安全性。
RECOVERY 是一项随机、对照、开放性平台试验,比较了 COVID-19 住院患者的几种可能治疗方法与常规护理。127 家英国医院参与了 casirivimab 和 imdevimab 的评估。合格的参与者是任何年龄至少 12 岁、因临床疑似或实验室确诊 SARS-CoV-2 感染而住院的患者。参与者被随机分配(1:1)接受常规标准护理或常规护理加 casirivimab 4g 和 imdevimab 4g 联合单次静脉输注。在试验过程中,调查人员和数据评估人员对结果数据的分析进行了屏蔽。主要结局是 28 天全因死亡率,按意向治疗进行评估,首次仅在随机分组时没有检测到 SARS-CoV-2 感染抗体的患者(即血清阴性)中进行评估,然后在总体人群中进行评估。所有接受 casirivimab 和 imdevimab 治疗的患者均进行了安全性评估。该试验在 ISRCTN(50189673)和 ClinicalTrials.gov(NCT04381936)上注册。
2020 年 9 月 18 日至 2021 年 5 月 22 日,RECOVERY 纳入了 9785 名符合条件的患者,他们可接受 casirivimab 和 imdevimab 治疗,其中 4839 名患者被随机分配接受 casirivimab 和 imdevimab 联合常规护理,4946 名患者接受常规护理。9785 名患者中,3153 名(32%)为血清阴性,5272 名(54%)为血清阳性,1360 名(14%)基线抗体状态未知。已知 812 名(8%)患者至少接受过一剂 SARS-CoV-2 疫苗。在血清阴性患者的主要疗效人群中,与接受常规护理的 1520 名患者相比,接受 casirivimab 和 imdevimab 治疗的 1633 名患者中有 396 名(24%)在 28 天内死亡(率比[RR]0.79,95%CI0.69-0.91;p=0.0009)。在所有随机分配的患者(无论基线抗体状态如何)的分析中,与接受常规护理的 4946 名患者相比,接受 casirivimab 和 imdevimab 治疗的 4839 名患者中有 943 名(19%)在 28 天内死亡(RR0.94,95%CI0.86-1.02;p=0.14)。casirivimab 和 imdevimab 对死亡率的影响比例在血清阳性和血清阴性患者之间有显著差异(异质性检验 p 值=0.002)。没有死亡归因于治疗,也没有在特定安全性结局(特定原因死亡率、心律失常、血栓形成或大出血事件)方面出现有意义的组间差异。在 7 名(<1%)参与者中报告的严重不良反应被当地研究者认为与接受 casirivimab 和 imdevimab 治疗有关。
在因 COVID-19 住院的患者中,casirivimab 和 imdevimab 联合应用于基线时血清阴性(因此没有产生自身体液免疫反应)的患者,降低了 28 天死亡率,但对基线时血清阳性的患者没有影响。
英国研究与创新署(医学研究理事会)和英国国家卫生研究院。