Yang Guanjie, Xie Jun, Guo Yadong, Yuan Jing, Wang Ruiliang, Guo Changcheng, Peng Bo, Yao Xudong, Yang Bin
Department of Urology, Shanghai Tenth People's Hospital, Tongji University School of Medicine, Shanghai, China.
Shanghai Clinical College, Anhui Medical University, Shanghai, China.
Front Oncol. 2022 Jan 26;11:790183. doi: 10.3389/fonc.2021.790183. eCollection 2021.
The therapeutic effect of extended pelvic lymph node dissection (PLND) in prostate cancer (PCa) patients is still controversial. The aim of this study was to identify the PCa patients who may benefit from extended PLND based on the 2012 Briganti nomogram.
PCa patients who underwent radical prostatectomy (RP) plus PLND between 2010 and 2015 were identified from the Surveillance, Epidemiology, and End Results (SEER) database. The probability of lymph node invasion (LNI), determined using the 2012 Briganti nomogram, was used to stratify the patients. The endpoints were overall survival (OS) and cancer-specific survival (CSS). Propensity score matching (PSM) was performed to account for potential differences between patients with and without extended PLND. Univariable and multivariable Cox regression was used to analyze the association between the number of removed nodes (NRN) and survival. Kaplan-Meier analysis was performed to estimate OS and CSS. Extended PLND was defined as NRN >75th percentile.
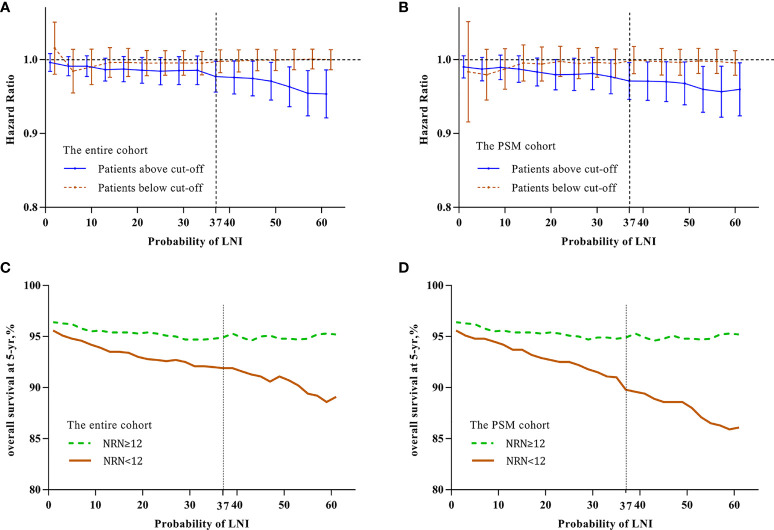
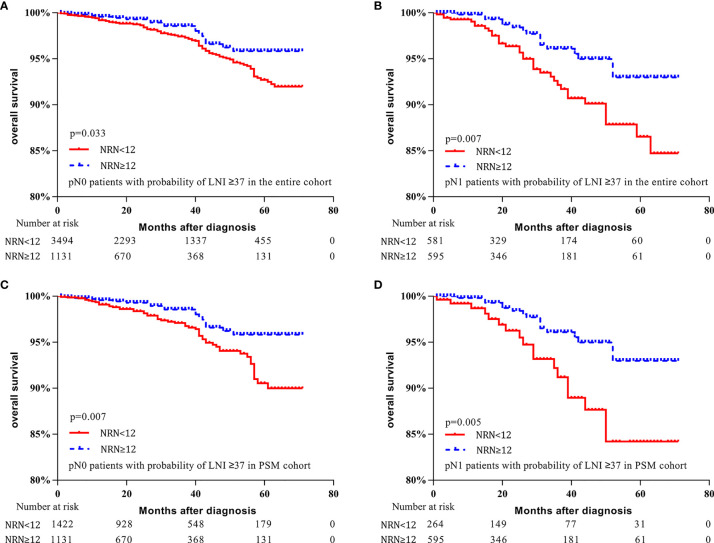
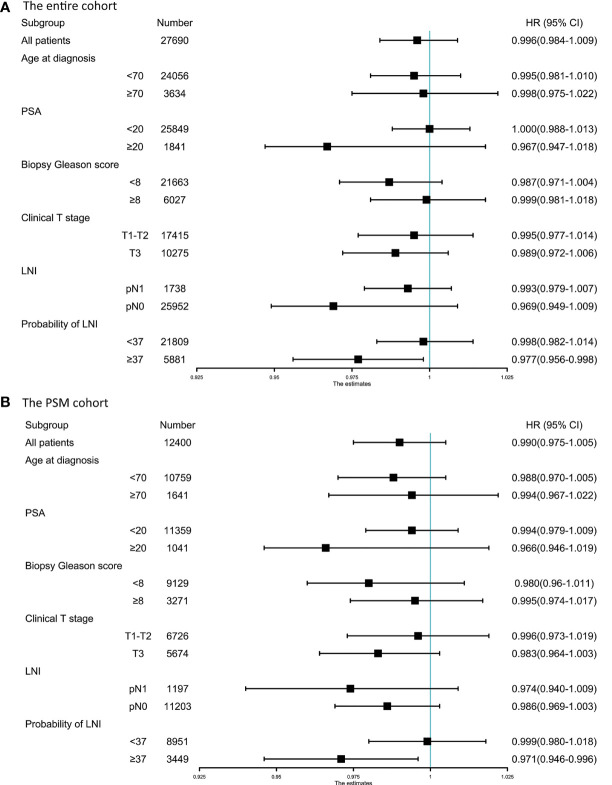
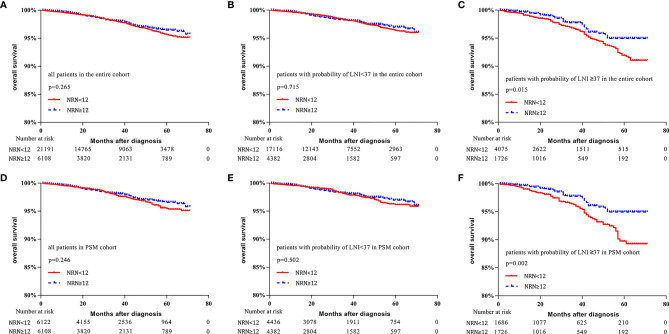
A total of 27,690 patients were included in the study. NRN was not an independent predictor of OS (p = 0.564). However, in patients with probability of LNI ≥37, multivariable analyses showed that increased NRN was associated with improved OS (hazard ratio [HR] = 0.963; p = 0.002). The 5-y OS rate was significantly higher for patients with NRN ≥12 than those with NRN <12 (94.9% vs. 91.9%, respectively; p = 0.015). In the PSM cohort, among patients with probability of LNI ≥37, multivariable analyses showed that increased NRN was associated with improved OS (HR = 0.961; p = 0.004). In addition, the 5-y OS rate was significantly higher for patients with NRN ≥12 than those with NRN <12 (94.9% vs. 89.8%, respectively; p = 0.002). However, NRN was not an independent predictor of CSS in any LNI risk subgroup (all p >0.05).
Extensive PLND might be associated with improved survival in PCa patients with a high risk of LNI, which supports the use of extended PLND in highly selected PCa patients. The results need to be validated in prospective studies with long-term follow-up.
扩大盆腔淋巴结清扫术(PLND)在前列腺癌(PCa)患者中的治疗效果仍存在争议。本研究的目的是基于2012年布里甘蒂列线图确定可能从扩大PLND中获益的PCa患者。
从监测、流行病学和最终结果(SEER)数据库中识别出2010年至2015年间接受根治性前列腺切除术(RP)加PLND的PCa患者。使用2012年布里甘蒂列线图确定的淋巴结转移(LNI)概率对患者进行分层。终点指标为总生存期(OS)和癌症特异性生存期(CSS)。进行倾向评分匹配(PSM)以消除接受和未接受扩大PLND患者之间的潜在差异。采用单变量和多变量Cox回归分析切除淋巴结数量(NRN)与生存期之间的关联。进行Kaplan-Meier分析以估计OS和CSS。扩大PLND定义为NRN>第75百分位数。
本研究共纳入27,690例患者。NRN不是OS的独立预测因素(p = 0.564)。然而,在LNI概率≥37的患者中,多变量分析显示NRN增加与OS改善相关(风险比[HR]=0.963;p = 0.002)。NRN≥12的患者5年OS率显著高于NRN<12的患者(分别为94.9%和91.9%;p = 0.015)。在PSM队列中,在LNI概率≥37的患者中,多变量分析显示NRN增加与OS改善相关(HR = 0.961;p = 0.004)。此外,NRN≥12的患者5年OS率显著高于NRN<12的患者(分别为94.9%和89.8%;p = 0.002)。然而,在任何LNI风险亚组中,NRN都不是CSS的独立预测因素(所有p>0.05)。
扩大PLND可能与LNI高风险的PCa患者生存期改善相关,这支持在经过严格筛选的PCa患者中使用扩大PLND。结果需要在前瞻性长期随访研究中进行验证。