Picariello Stefania, Cerbone Manuela, D'Arco Felice, Gan Hoong-Wei, O'Hare Patricia, Aquilina Kristian, Opocher Enrico, Hargrave Darren, Spoudeas Helen A
Neuro-Oncology Unit, Department of Paediatric Oncology, Santobono-Pausilipon Children's Hospital, 80123 Naples, Italy.
Department of Woman, Child and General and Specialized Surgery, University of Campania Luigi Vanvitelli, 80138 Naples, Italy.
Cancers (Basel). 2022 Jan 31;14(3):747. doi: 10.3390/cancers14030747.
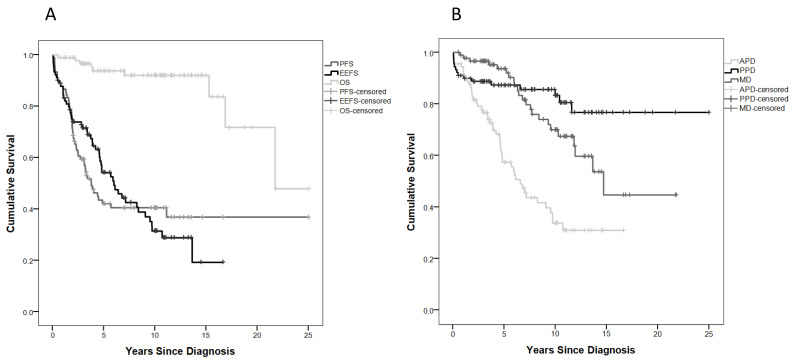
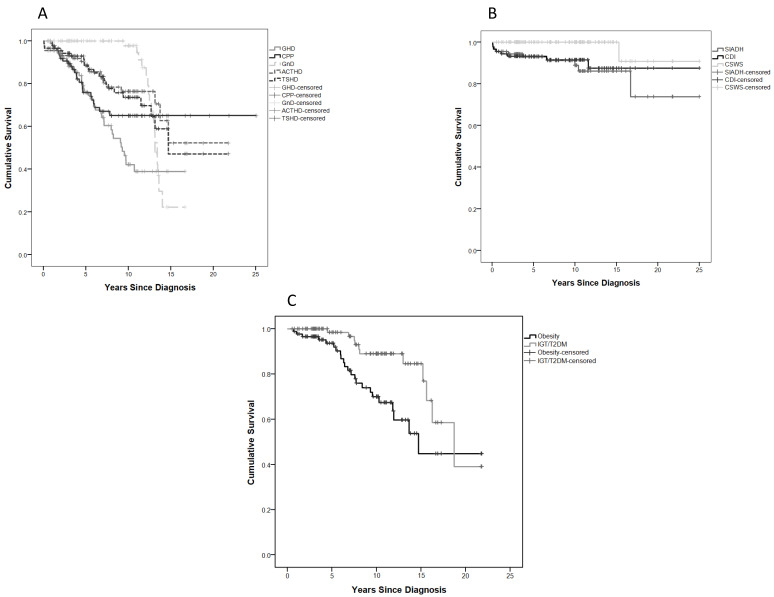
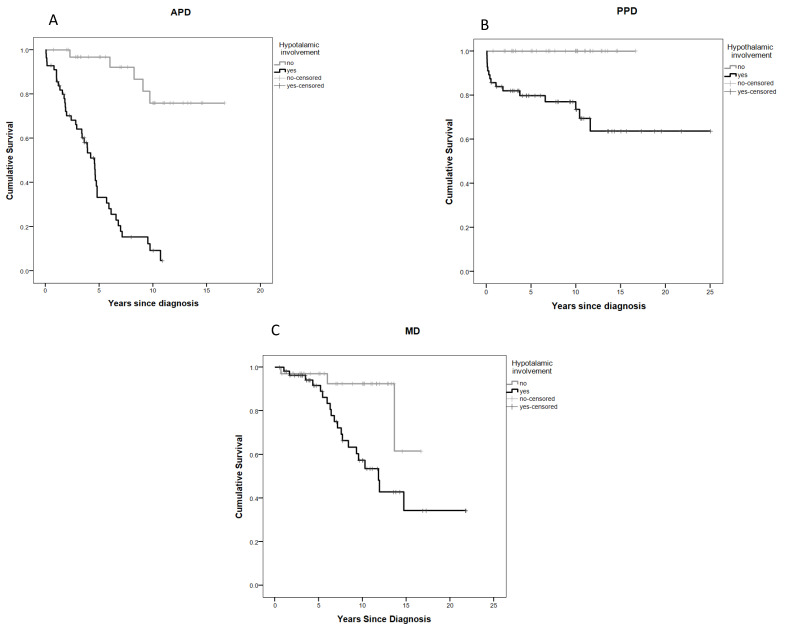
Despite high survival, paediatric optic pathway hypothalamic gliomas are associated with significant morbidity and late mortality. Those youngest at presentation have the worst outcomes. We aimed to assess presenting disease, tumour location, and treatment factors implicated in the evolution of neuroendocrine, metabolic, and neurobehavioural morbidity in 90 infants/children diagnosed before their third birthday and followed-up for 9.5 years (range 0.5-25.0). A total of 52 (57.8%) patients experienced endo-metabolic dysfunction (EMD), the large majority (46) of whom had hypothalamic involvement (H+) and lower endocrine event-free survival (EEFS) rates. EMD was greatly increased by a diencephalic syndrome presentation (85.2% vs. 46%, = 0.001)), H+ (OR 6.1 95% CI 1.7-21.7, 0.005), radiotherapy (OR 16.2, 95% CI 1.7-158.6, = 0.017) and surgery (OR 4.8 95% CI 1.3-17.2, = 0.015), all associated with anterior pituitary disorders. Obesity occurred in 25% of cases and was clustered with the endocrinopathies. Neurobehavioural deficits occurred in over half (52) of the cohort and were associated with H+ (OR 2.5 95% C.I. 1.1-5.9, = 0.043) and radiotherapy (OR 23.1 C.I. 2.9-182, = 0.003). Very young children with OPHG carry a high risk of endo-metabolic and neurobehavioural comorbidities which deserve better understanding and timely/parallel support from diagnosis to improve outcomes. These evolve in complex, hierarchical patterns over time whose aetiology appears predominantly determined by injury from the hypothalamic tumour location alongside adjuvant treatment strategies.
尽管小儿视神经通路下丘脑胶质瘤的生存率较高,但仍伴有显著的发病率和晚期死亡率。就诊时年龄最小的患儿预后最差。我们旨在评估90例在3岁前确诊并随访9.5年(范围0.5 - 25.0年)的婴儿/儿童的就诊疾病、肿瘤位置以及与神经内分泌、代谢和神经行为发病率演变相关的治疗因素。共有52例(57.8%)患者出现内分泌 - 代谢功能障碍(EMD),其中绝大多数(46例)有下丘脑受累(H +)且内分泌无事件生存率(EEFS)较低。双相性精神障碍表现会显著增加EMD的发生几率(85.2%对46%,P = 0.001),H +(比值比6.1,95%置信区间1.7 - 21.7,P = 0.005)、放疗(比值比16.2,95%置信区间1.7 - 158.6,P = 0.017)和手术(比值比4.8,95%置信区间1.3 - 17.2,P = 0.015)也会增加EMD发生几率,所有这些都与垂体前叶疾病有关。25%的病例出现肥胖,且与内分泌疾病聚集。超过一半(52例)的队列出现神经行为缺陷,这与H +(比值比2.5,95%置信区间1.1 - 5.9,P = 0.043)和放疗(比值比23.1,置信区间2.9 - 182,P = 0.003)有关。患有视神经通路下丘脑胶质瘤的幼儿发生内分泌 - 代谢和神经行为合并症的风险很高,这值得更好地理解,并在诊断后及时/同时给予支持以改善预后。这些合并症会随着时间以复杂的层级模式演变,其病因似乎主要由下丘脑肿瘤位置的损伤以及辅助治疗策略决定。