UniSA: School of Pharmacy and Medical Science, Clinical and Health Sciences, University of South Australia, Adelaide, Australia.
Pharmacy Department, Mohammed Almana College for Medical Sciences, Abdulrazaq Bin Hammam Street, Alsafa, Dammam, Saudi Arabia.
Eur J Drug Metab Pharmacokinet. 2022 May;47(3):387-402. doi: 10.1007/s13318-022-00756-x. Epub 2022 Feb 15.
Tramadol is commonly prescribed to manage chronic pain in older patients. However, there is a gap in the literature describing the pharmacokinetic parameters for tramadol and its active metabolite (O-desmethyltramadol [ODT]) in this population. The objective of this study was to develop and evaluate a population pharmacokinetic model for tramadol and ODT in older patients.
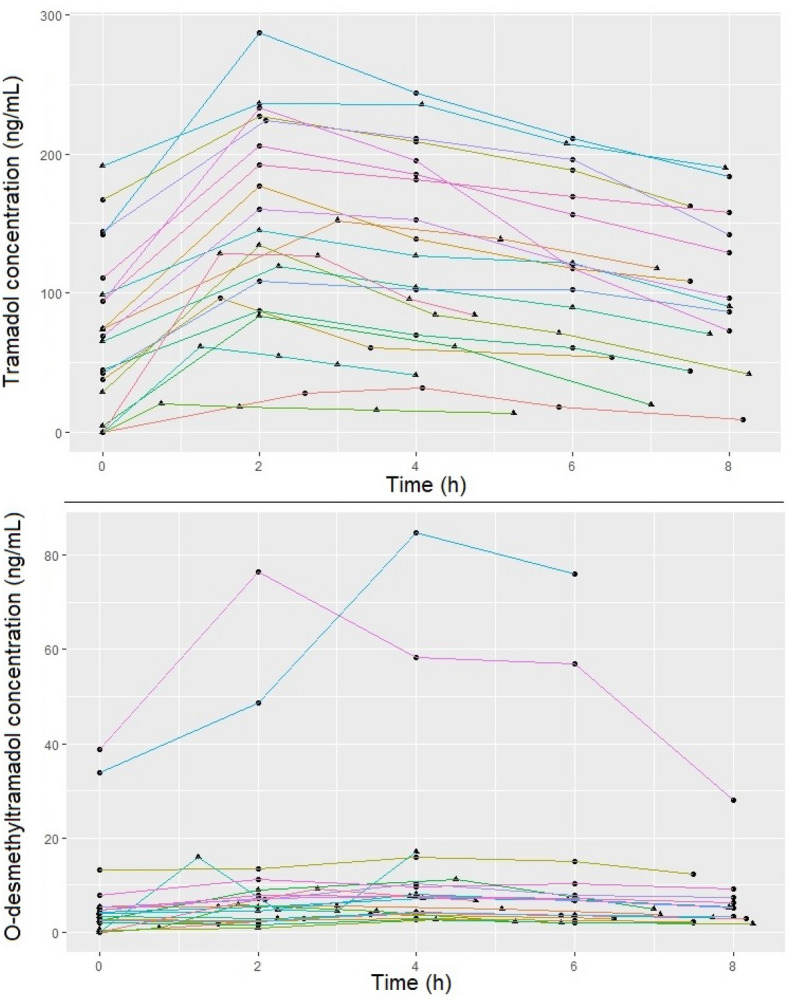
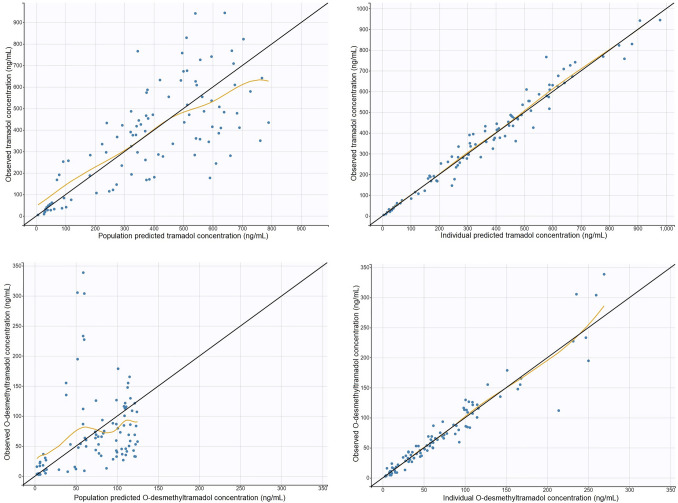
Twenty-one patients who received an extended-release oral tramadol dose (25-100 mg) were recruited. Tramadol and ODT concentrations were determined using a validated liquid chromatography/tandem mass spectrometry method. A population pharmacokinetic model was developed using non-linear mixed-effects modelling. The performance of the model was assessed by visual predictive check.
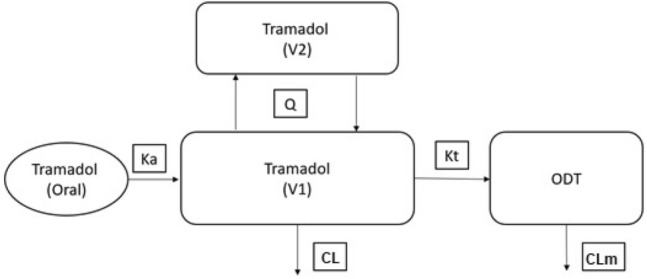
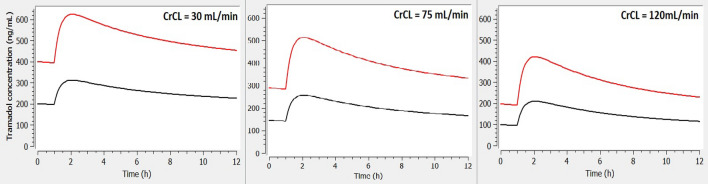
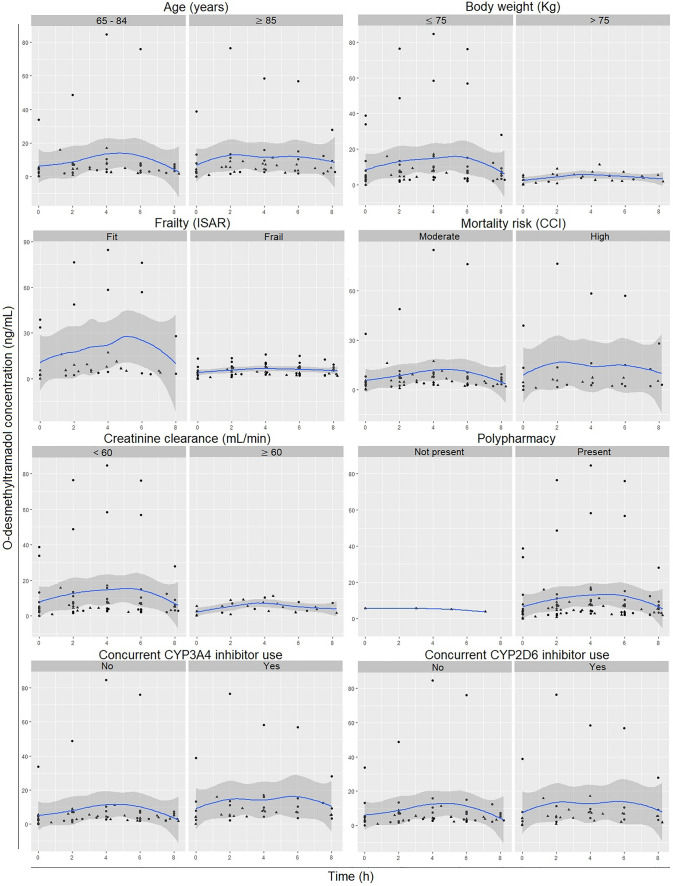
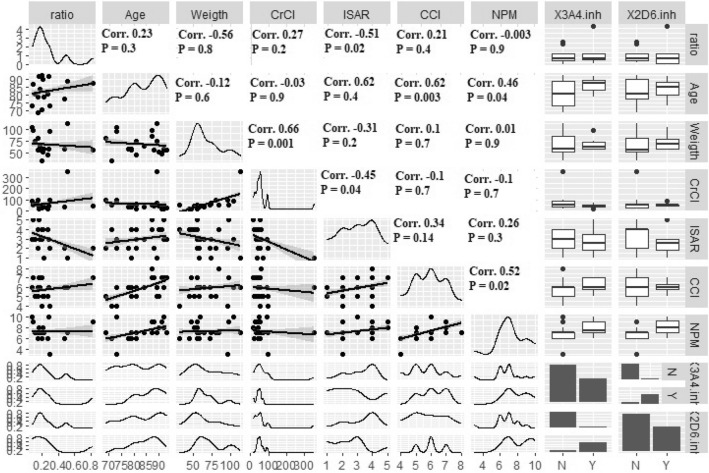
A two-compartment, first-order absorption model with linear elimination best described the tramadol concentration data. The absorption rate constant was 2.96/h (between-subject variability [BSV] 37.8%), apparent volume of distribution for the central compartment (V/F) was 0.373 l (73.8%), apparent volume of distribution for the peripheral compartment (V/F) was 0.379 l (97.4%), inter-compartmental clearance (Q) was 0.0426 l/h (2.19%) and apparent clearance (CL/F) was 0.00604 l/h (6.61%). The apparent rate of metabolism of tramadol to ODT (k) was 0.0492 l/h (78.5%) and apparent clearance for ODT (CL) was 0.143 l/h (21.6%). Identification of Seniors at Risk score (ISAR) and creatinine clearance (CrCL) were the only covariates included in the final model, where a higher value for the ISAR increased the maximum concentration (C) of tramadol and reduced the BSV in Q from 4.71 to 2.19%. A higher value of CrCL reduced tramadol C and half-life (T) and reduced the BSV in V/F (from 148 to 97.4%) and in CL/F (from 78.9 to 6.61%).
Exposure to tramadol increased with increased frailty and reduced CrCL. Prescribers should consider patients frailty status and CrCL to minimise the risk of tramadol toxicity in such cohort of patients.
曲马多常用于治疗老年患者的慢性疼痛。然而,文献中对于该人群中曲马多及其活性代谢物(O-去甲基曲马多[ODT])的药代动力学参数存在差距。本研究旨在建立和评估老年患者曲马多和 ODT 的群体药代动力学模型。
招募了 21 名接受缓释口服曲马多剂量(25-100mg)的患者。使用经过验证的液相色谱/串联质谱法测定曲马多和 ODT 浓度。使用非线性混合效应模型建立群体药代动力学模型。通过视觉预测检查评估模型的性能。
一个两室、一级吸收模型,具有线性消除,最能描述曲马多浓度数据。吸收速率常数为 2.96/h(个体间变异度[BSV]为 37.8%),中央室表观分布容积(V/F)为 0.373l(73.8%),外周室表观分布容积(V/F)为 0.379l(97.4%),隔室清除率(Q)为 0.0426l/h(2.19%),表观清除率(CL/F)为 0.00604l/h(6.61%)。曲马多转化为 ODT 的表观代谢率(k)为 0.0492l/h(78.5%),ODT 表观清除率(CL)为 0.143l/h(21.6%)。老年人风险识别评分(ISAR)和肌酐清除率(CrCL)是最终模型中唯一包含的协变量,ISAR 值较高会增加曲马多的最大浓度(C),并将 Q 的 BSV 从 4.71 降低到 2.19%。CrCL 值较高会降低曲马多的 C 和半衰期(T),并降低 V/F(从 148 降低到 97.4%)和 CL/F(从 78.9 降低到 6.61%)的 BSV。
曲马多的暴露量随着脆弱性的增加和 CrCL 的降低而增加。对于此类患者群体,临床医生应考虑患者的脆弱性状态和 CrCL,以尽量降低曲马多毒性的风险。