Xu San San, Sinclair Nicholas C, Bulluss Kristian J, Perera Thushara, Lee Wee-Lih, McDermott Hugh J, Thevathasan Wesley
Bionics Institute, East Melbourne, VIC, Australia.
Brain Commun. 2022 Jan 13;4(1):fcac003. doi: 10.1093/braincomms/fcac003. eCollection 2022.
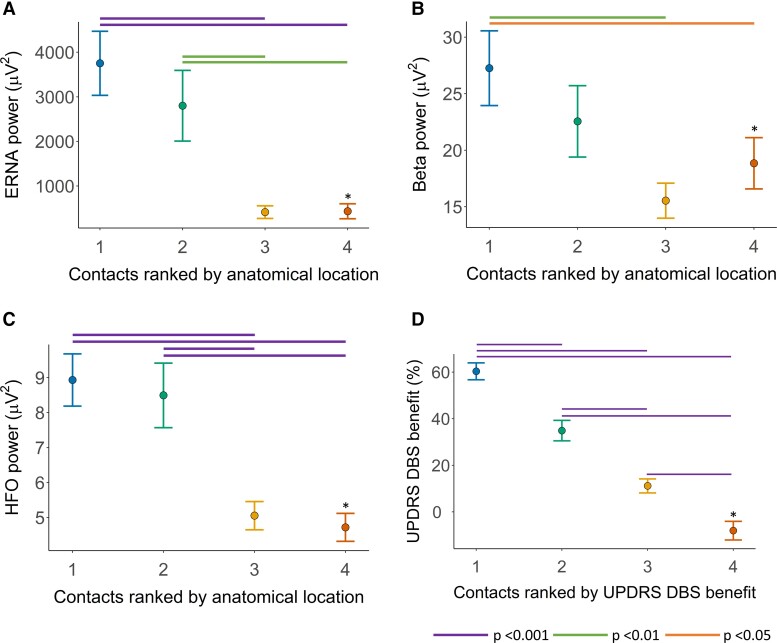
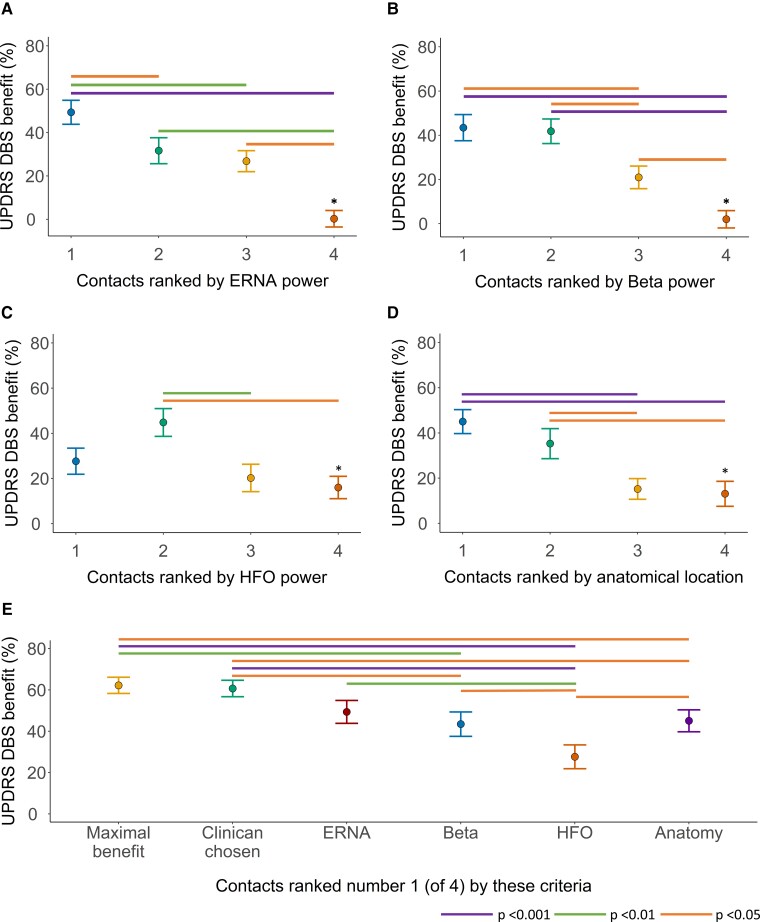
Selecting the ideal contact to apply subthalamic nucleus deep brain stimulation in Parkinson's disease can be an arduous process, with outcomes highly dependent on clinician expertise. This study aims to assess whether neuronal signals recorded intraoperatively in awake patients, and the anatomical location of contacts, can assist programming. In a cohort of 14 patients with Parkinson's disease, implanted with subthalamic nucleus deep brain stimulation, the four contacts on each lead in the 28 hemispheres were ranked according to proximity to a nominated ideal anatomical location and power of the following neuronal signals: evoked resonant neural activity, beta oscillations and high-frequency oscillations. We assessed how these rankings predicted, on each lead: (i) the motor benefit from deep brain stimulation applied through each contact and (ii) the 'ideal' contact to apply deep brain stimulation. The ranking of contacts according to each factor predicted motor benefit from subthalamic nucleus deep brain stimulation, as follows: evoked resonant neural activity; = 0.50, Akaike information criterion 1039.9, beta; = 0.50, Akaike information criterion 1041.6, high-frequency oscillations; = 0.44, Akaike information criterion 1057.2 and anatomy; = 0.49, Akaike information criterion 1048.0. Combining evoked resonant neural activity, beta and high-frequency oscillations ranking data yielded the strongest predictive model ( = 0.61, Akaike information criterion 1021.5). The 'ideal' contact (yielding maximal benefit) was ranked first according to each factor in the following proportion of hemispheres; evoked resonant neural activity 18/28, beta 17/28, anatomy 16/28, high-frequency oscillations 7/28. Across hemispheres, the maximal available deep brain stimulation benefit did not differ from that yielded by contacts chosen by clinicians for chronic therapy or contacts ranked first according to evoked resonant neural activity. Evoked resonant neural activity, beta oscillations and anatomy similarly predicted how motor benefit from subthalamic nucleus deep brain stimulation varied across contacts on each lead. This could assist programming by providing a probability ranking of contacts akin to a 'monopolar survey'. However, these factors identified the 'ideal' contact in only a proportion of hemispheres. More advanced signal processing and anatomical techniques may be needed for the full automation of contact selection.
选择理想的触点以在帕金森病中应用丘脑底核深部脑刺激可能是一个艰巨的过程,其结果高度依赖于临床医生的专业知识。本研究旨在评估清醒患者术中记录的神经元信号以及触点的解剖位置是否有助于编程。在一组14例植入丘脑底核深部脑刺激的帕金森病患者中,对28个半球中每根导线的4个触点根据与指定的理想解剖位置的接近程度以及以下神经元信号的功率进行排序:诱发共振神经活动、β振荡和高频振荡。我们评估了这些排序如何在每根导线上预测:(i) 通过每个触点施加深部脑刺激所带来的运动益处,以及(ii) 施加深部脑刺激的“理想”触点。根据每个因素对触点进行的排序预测了丘脑底核深部脑刺激带来的运动益处,如下所示:诱发共振神经活动;r = 0.50,赤池信息准则1039.9,β;r = 0.50,赤池信息准则1041.6,高频振荡;r = 0.44,赤池信息准则1057.2,解剖结构;r = 0.49,赤池信息准则1048.0。将诱发共振神经活动、β和高频振荡的排序数据相结合产生了最强的预测模型(r = 0.61,赤池信息准则1021.5)。在以下比例的半球中,“理想”触点(产生最大益处)根据每个因素被排在第一位;诱发共振神经活动18/28,β 17/28,解剖结构16/28,高频振荡7/28。在各个半球中,最大可用的深部脑刺激益处与临床医生选择用于长期治疗的触点或根据诱发共振神经活动排在第一位的触点所产生的益处没有差异。诱发共振神经活动、β振荡和解剖结构同样预测了丘脑底核深部脑刺激带来的运动益处在每根导线上的各个触点之间的变化情况。这可以通过提供类似于“单极测量”的触点概率排序来辅助编程。然而,这些因素仅在一部分半球中识别出了“理想”触点。可能需要更先进的信号处理和解剖技术来实现触点选择的完全自动化。