Sun Daokun, Schaff Hartzell V, Nishimura Rick A, Geske Jeffrey B, Dearani Joseph A, Ommen Steve R
Department of Cardiovascular Surgery, Mayo Clinic, Rochester, Minn.
Department of Cardiovascular Medicine, Mayo Clinic, Rochester, Minn.
JTCVS Tech. 2021 Nov 1;11:21-26. doi: 10.1016/j.xjtc.2021.10.050. eCollection 2022 Feb.
Some patients with obstructive hypertrophic cardiomyopathy may remain limited after surgical relief of the subaortic obstruction. In this report, we describe experience in surgical management of patients with advanced diastolic heart failure symptoms after adequate transaortic septal myectomy for obstructive hypertrophic cardiomyopathy.
We identified adult patients who presented with heart failure symptoms after previous transaortic septal myectomy for obstructive hypertrophic cardiomyopathy and underwent repeat sternotomy for transapical myectomy to enlarge a small left ventricular cavity. Functional recovery after hospital dismissal was assessed through a questionnaire-based survey.
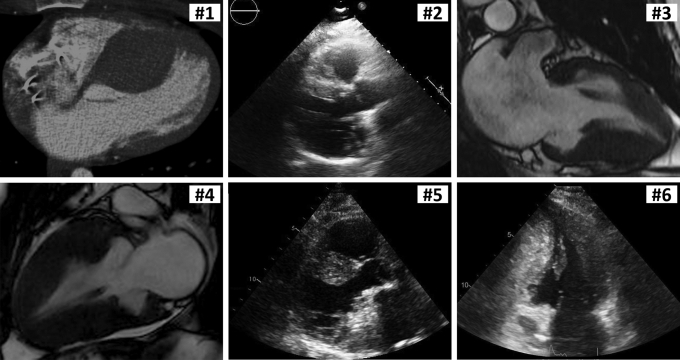
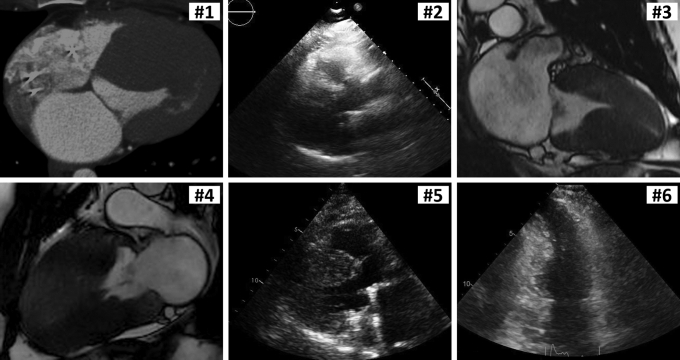
Six patients with previous septal myectomy presented with New York Heart Association functional class III symptoms. Preoperative transthoracic Doppler echocardiography confirmed adequate relief of subaortic outflow tract obstruction with only trivial or mild mitral valve regurgitation; left atrial volume index was increased at 46 mL/m (range, 44-47 mL/m). Following transapical myectomy, the left ventricular diameter was enlarged from 23 mm (range, 21-27 mm) to 29 mm (range, 27-31 mm) at end-systole and from 40 mm (range, 38-42 mm) to 43 mm (range, 42-50 mm) at end-diastole. All the patients were alive after a median follow-up of 0.6 years (range, 0.4-3.5 years), and 5 patients responded to a postoperative survey and indicated improvement in their heart condition compared with functional status before the repeat myectomy.
Patients with diastolic heart failure after septal myectomy for obstructive hypertrophic cardiomyopathy may present with systolic cavity obliteration due to excessive myocardial hypertrophy. Repeat transapical myectomy can enlarge the left ventricular chamber and augment the diastolic volume, which results in improved physical capacity and patient-perceived functional status.
一些梗阻性肥厚型心肌病患者在主动脉瓣下梗阻手术解除后仍可能存在功能受限。在本报告中,我们描述了对梗阻性肥厚型心肌病患者在进行充分的经主动脉间隔心肌切除术后出现晚期舒张性心力衰竭症状的手术治疗经验。
我们确定了成年患者,这些患者在先前因梗阻性肥厚型心肌病接受经主动脉间隔心肌切除术后出现心力衰竭症状,并接受了经心尖心肌切除术的再次开胸手术以扩大小的左心室腔。出院后的功能恢复通过基于问卷的调查进行评估。
6例先前接受间隔心肌切除术的患者出现纽约心脏协会功能分级III级症状。术前经胸多普勒超声心动图证实主动脉瓣下流出道梗阻得到充分缓解,仅存在微量或轻度二尖瓣反流;左心房容积指数增加至4� mL/m²(范围为44-47 mL/m²)。经心尖心肌切除术后,左心室直径在收缩末期从23毫米(范围为21-27毫米)扩大至29毫米(范围为27-31毫米),在舒张末期从40毫米(范围为38-42毫米)扩大至43毫米(范围为42-50毫米)。所有患者在中位随访0.6年(范围为0.4-3.5年)后均存活,5例患者对术后调查做出回应,并表示与再次心肌切除术前的功能状态相比,心脏状况有所改善。
梗阻性肥厚型心肌病间隔心肌切除术后出现舒张性心力衰竭的患者可能因心肌过度肥厚而出现收缩期心室腔闭塞。再次经心尖心肌切除术可扩大左心室腔并增加舒张容积,从而改善体能和患者自我感知的功能状态。