Department of Cardiovascular Surgery, Osaka City University Graduate School of Medicine, 1-4-3 Asahimachi, Abeno, Osaka, 545-8585, Japan.
J Cardiothorac Surg. 2022 Feb 16;17(1):18. doi: 10.1186/s13019-022-01762-5.
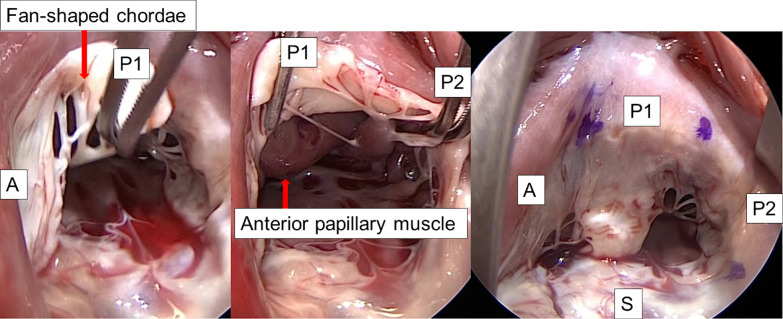
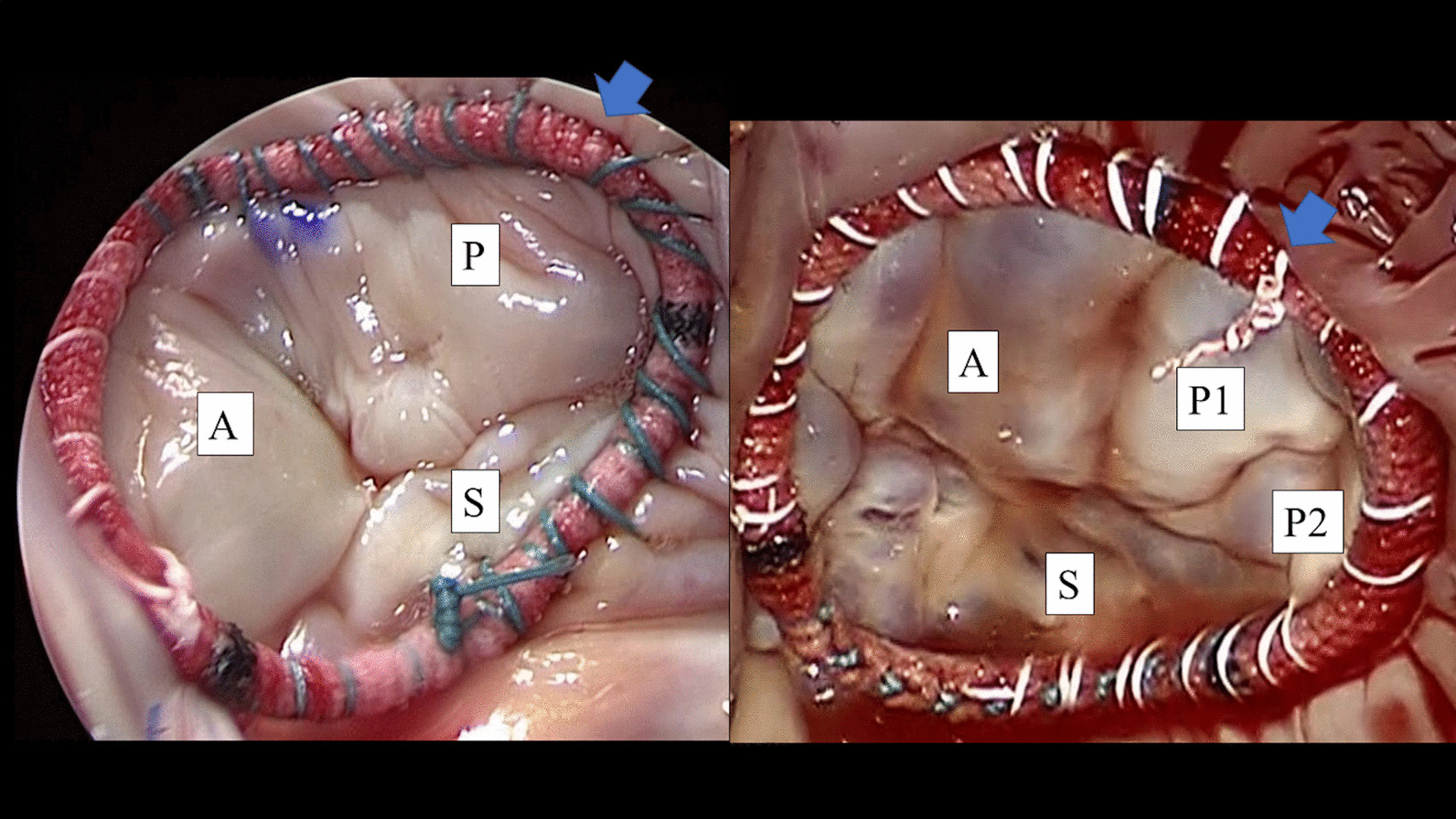
We investigated the effect of morphological diversity of the tricuspid valve with multiple posterior leaflets on the technical outcomes of tricuspid valve repair.
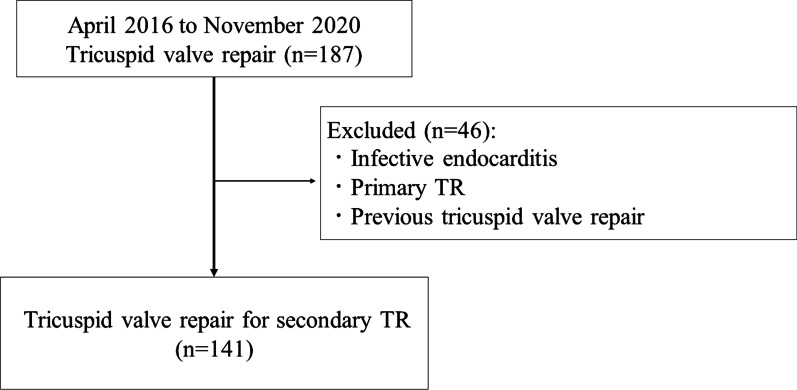
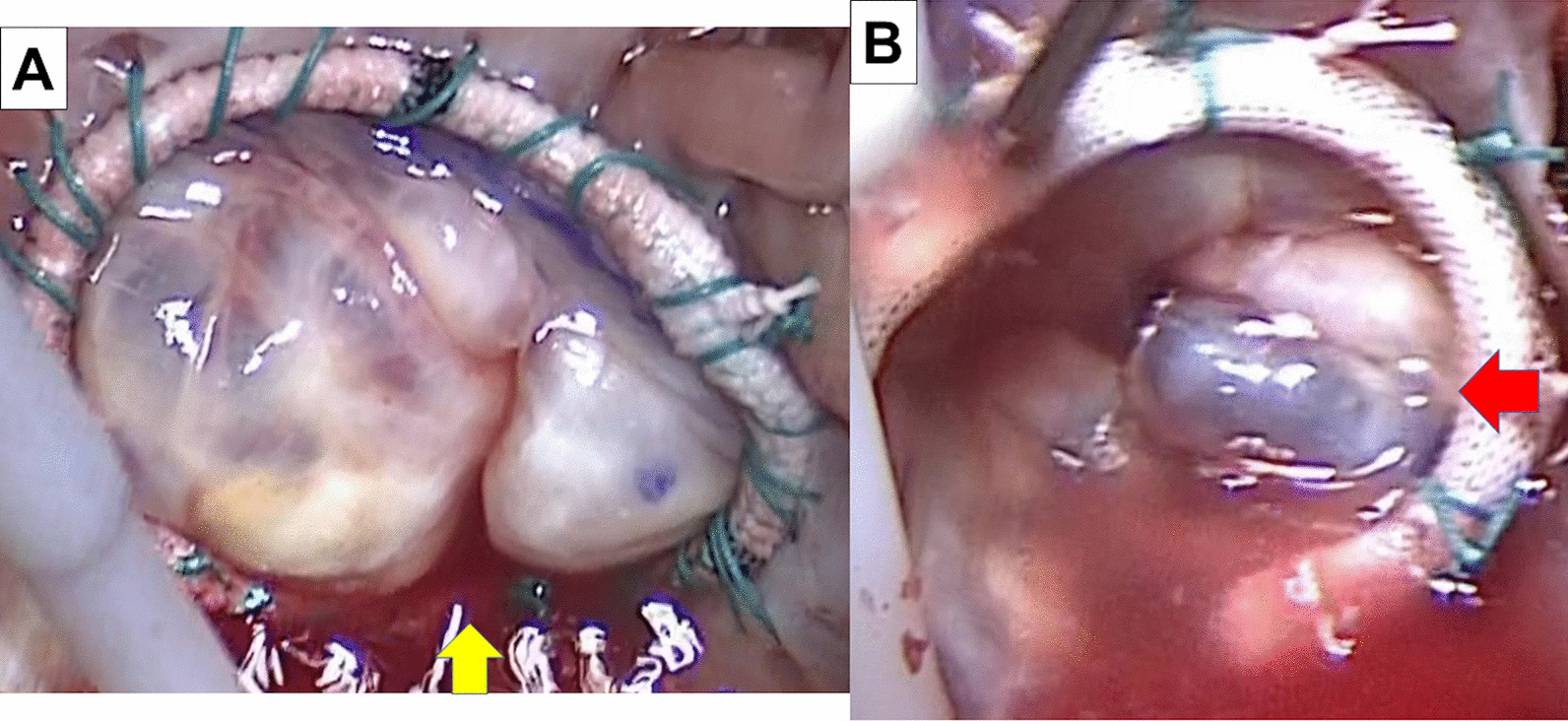
From April 2016 to November 2020, 141 patients were diagnosed with secondary tricuspid regurgitation associated with left heart disease and underwent tricuspid valve repair. We retrospectively analyzed the clinical and echocardiographic data of patients who underwent both preoperative and postoperative transthoracic echocardiography. We divided the patients into two groups according to the surgical technique used to treat tricuspid regurgitation: ring annuloplasty alone (Group 1, n = 109) or additional approximation of leaflet edges (edge-to-edge repair) with ring annuloplasty (Group 2, n = 32). We measured the morphological diversity of the tricuspid valve during the operation in all patients.
The preoperative tricuspid regurgitation score was higher in Group 2 than in Group 1 (2.1 ± 0.78 vs. 1.6 ± 0.7, respectively; p = 0.0046), and Group 2 contained more patients with two posterior leaflets than Group 1 [20 (63%) vs. 36 (33%), respectively; p = 0.003]. The univariate and multivariate logistic regression analyses showed that the presence of two posterior leaflets was an independent risk factor for additional procedures during tricuspid valve repair (odds ratio, 2.6; 95% confidence interval, 1.1-6.1; p = 0.033).
Additional procedures to reduce tricuspid regurgitation were required more frequently in patients with two posterior leaflets of the tricuspid valve. The morphological diversity of two posterior leaflets is a potential risk factor for a more complicated tricuspid repair.
研究三尖瓣多个后瓣叶的形态多样性对三尖瓣修复技术结果的影响。
2016 年 4 月至 2020 年 11 月,141 例诊断为左心疾病相关继发性三尖瓣反流的患者接受了三尖瓣修复术。我们回顾性分析了所有接受术前和术后经胸超声心动图检查的患者的临床和超声心动图数据。我们根据治疗三尖瓣反流的手术技术将患者分为两组:单纯环成形术(第 1 组,n=109)或环成形术联合瓣缘靠拢术(边对边修复,第 2 组,n=32)。我们在所有患者的手术过程中测量三尖瓣的形态多样性。
第 2 组患者的术前三尖瓣反流评分高于第 1 组(2.1±0.78 比 1.6±0.7,分别;p=0.0046),第 2 组有更多的患者有两个后瓣叶(20[63%]比 36[33%],分别;p=0.003)。单因素和多因素逻辑回归分析显示,两个后瓣叶的存在是三尖瓣修复术时需要附加手术的独立危险因素(比值比,2.6;95%置信区间,1.1-6.1;p=0.033)。
三尖瓣有两个后瓣叶的患者需要更频繁地进行额外的减少三尖瓣反流的手术。两个后瓣叶的形态多样性是三尖瓣修复更复杂的潜在危险因素。