Harvard Medical School, Boston, Massachusetts.
Department of Medicine, Massachusetts General Hospital, Boston.
JAMA Netw Open. 2022 Feb 1;5(2):e220354. doi: 10.1001/jamanetworkopen.2022.0354.
COVID-19 has disproportionately killed older adults and racial and ethnic minority individuals, raising questions about the relevance of advance care planning (ACP) in this population. Video decision aids and communication skills training offer scalable delivery models.
To assess whether ACP video decision aids and a clinician communication intervention improved the rate of ACP documentation during an evolving pandemic, with a focus on African American and Hispanic patients.
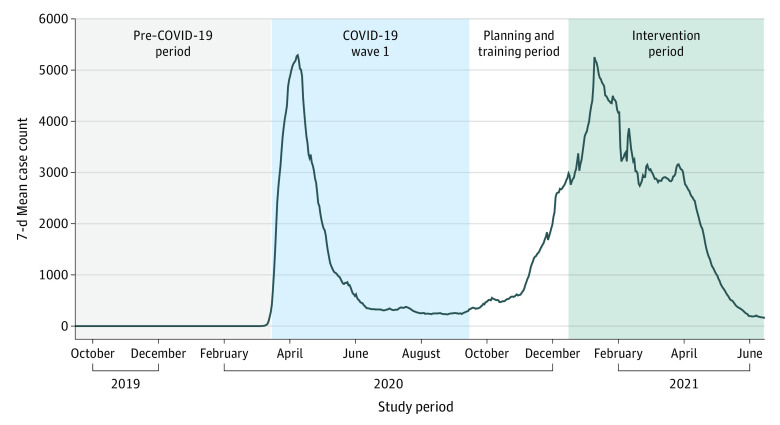
DESIGN, SETTING, AND PARTICIPANTS: The Advance Care Planning: Communicating With Outpatients for Vital Informed Decisions trial was a pre-post, open-cohort nonrandomized controlled trial that compared ACP documentation across the baseline pre-COVID-19 period (September 15, 2019, to March 14, 2020), the COVID-19 wave 1 period (March 15, 2020, to September 14, 2020), and an intervention period (December 15, 2020, to June 14, 2021) at a New York metropolitan area ambulatory network of 22 clinics. All patients 65 years or older who had at least 1 clinic or telehealth visit during any of the 3 study periods were included.
The primary outcome was ACP documentation.
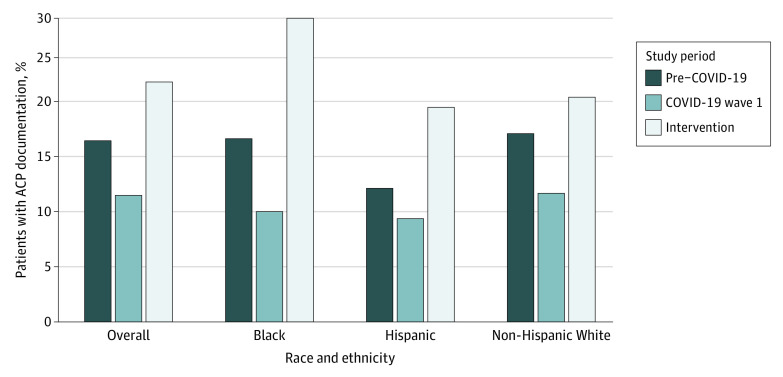
A total of 14 107 patients (mean [SD] age, 81.0 [8.4] years; 8856 [62.8%] female; and 2248 [15.9%] African American or Hispanic) interacted with clinicians during the pre-COVID-19 period; 12 806 (mean [SD] age, 81.2 [8.5] years; 8047 [62.8%] female; and 1992 [15.6%] African American or Hispanic), during wave 1; and 15 106 (mean [SD] 80.9 [8.3] years; 9543 [63.2%] female; and 2535 [16.8%] African American or Hispanic), during the intervention period. Clinicians documented ACP in 3587 patients (23.8%) during the intervention period compared with 2525 (17.9%) during the pre-COVID-19 period (rate difference [RD], 5.8%; 95% CI, 0.9%-7.9%; P = .01) and 1598 (12.5%) during wave 1 (RD, 11.3%; 95% CI, 6.3%-12.1%; P < .001). Advance care planning was documented in 447 African American patients (30.0%) during the intervention period compared with 233 (18.1%) during the pre-COVID-19 period (RD, 11.9%; 95% CI, 4.1%-15.9%; P < .001) and 130 (11.0%) during wave 1 (RD, 19.1%; 95% CI, 11.7%-21.2%; P < .001). Advance care planning was documented for 222 Hispanic patients (21.2%) during the intervention period compared with 127 (13.2%) during the pre-COVID-19 period (RD, 8.0%; 95% CI, 2.1%-10.9%; P = .004) and 82 (10.2%) during wave 1 (RD, 11.1%; 95% CI, 5.5%-14.5%; P < .001).
This intervention, implemented during the evolving COVID-19 pandemic, was associated with higher rates of ACP documentation, especially for African American and Hispanic patients.
ClinicalTrials.gov Identifier: NCT04660422.
COVID-19 对老年人和少数族裔造成了不成比例的影响,这引发了关于在这一人群中进行预先护理计划(ACP)的相关性问题。视频决策辅助工具和沟通技巧培训提供了可扩展的交付模式。
评估 ACP 视频决策辅助工具和临床医生沟通干预措施是否可以提高在不断演变的大流行期间 ACP 记录的比率,重点关注非裔美国人和西班牙裔患者。
设计、地点和参与者:Advance Care Planning: Communicating With Outpatients for Vital Informed Decisions 试验是一项前后、开放队列、非随机对照试验,比较了在基线期 COVID-19 前(2019 年 9 月 15 日至 2020 年 3 月 14 日)、COVID-19 第 1 波(2020 年 3 月 15 日至 2020 年 9 月 14 日)和干预期(2020 年 12 月 15 日至 2021 年 6 月 14 日)期间,在纽约都会区的 22 个诊所的门诊网络中进行 ACP 记录。所有在任何 3 个研究期间至少有 1 次诊所或远程医疗就诊的 65 岁及以上患者都包括在内。
主要结果是 ACP 记录。
共有 14107 名患者(平均[标准差]年龄,81.0[8.4]岁;8856 名[62.8%]女性;2248 名[15.9%]非裔美国人或西班牙裔)在 COVID-19 前期间与临床医生进行了互动;12806 名(平均[标准差]年龄,81.2[8.5]岁;8047 名[62.8%]女性;1992 名[15.6%]非裔美国人和西班牙裔)在第 1 波期间;15106 名(平均[标准差]80.9[8.3]岁;9543 名[63.2%]女性;2535 名[16.8%]非裔美国人和西班牙裔)在干预期间。与 COVID-19 前期间(记录率差异[RD],5.8%;95%CI,0.9%-7.9%;P=0.01)和第 1 波期间(RD,11.3%;95%CI,6.3%-12.1%;P<0.001)相比,临床医生在干预期间记录了 3587 名患者(23.8%)的 ACP,在 COVID-19 前期间记录了 2525 名(17.9%),在第 1 波期间记录了 1598 名(12.5%)。在干预期间,447 名非裔美国患者(30.0%)记录了 ACP,而在 COVID-19 前期间记录了 233 名(18.1%)(RD,11.9%;95%CI,4.1%-15.9%;P<0.001),在第 1 波期间记录了 130 名(11.0%)(RD,19.1%;95%CI,11.7%-21.2%;P<0.001)。在干预期间,222 名西班牙裔患者(21.2%)记录了 ACP,而在 COVID-19 前期间记录了 127 名(13.2%)(RD,8.0%;95%CI,2.1%-10.9%;P=0.004),在第 1 波期间记录了 82 名(10.2%)(RD,11.1%;95%CI,5.5%-14.5%;P<0.001)。
在不断演变的 COVID-19 大流行期间实施的这一干预措施与 ACP 记录率的提高有关,特别是针对非裔美国人和西班牙裔患者。
ClinicalTrials.gov 标识符:NCT04660422。