Ng Tat Ming, Ong Sean W X, Loo Audrey Y X, Tan Sock Hoon, Tay Hui Lin, Yap Min Yi, Lye David C, Lee Tau Hong, Young Barnaby E
Department of Pharmacy, Tan Tock Seng Hospital, 11 Jalan Tan Tock Seng, Singapore 308433, Singapore.
Department of Infectious Diseases, National Centre for Infectious Diseases, 16 Jln Tan Tock Seng, Singapore 308442, Singapore.
Antibiotics (Basel). 2022 Jan 31;11(2):184. doi: 10.3390/antibiotics11020184.
COVID-19 imposes challenges in antibiotic decision-making due to similarities between bacterial pneumonia and moderate to severe COVID-19. We evaluated the effects of antibiotic therapy on the clinical outcomes of COVID-19 pneumonia patients and diagnostic accuracy of key inflammatory markers to inform antibiotic decision-making.
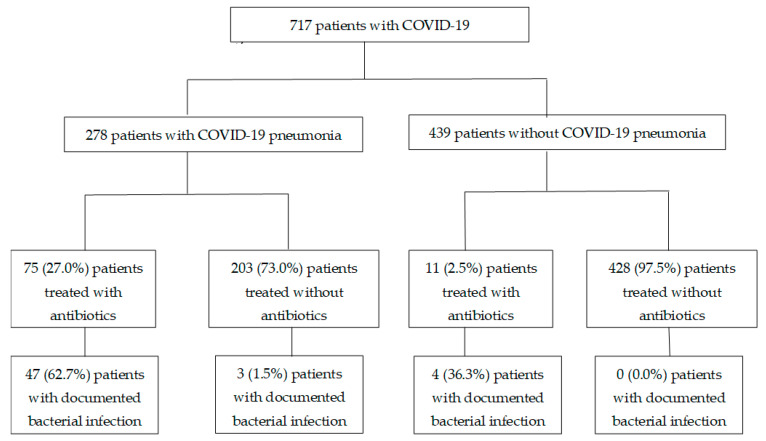
An observational cohort study was conducted in patients hospitalised with COVID-19 at the National Centre for Infectious Diseases and Tan Tock Seng Hospital, Singapore, from January to April 2020. Patients were defined as receiving empiric antibiotic treatment for COVID-19 if started within 3 days of diagnosis.
Of 717 patients included, 86 (12.0%) were treated with antibiotics and 26 (3.6%) had documented bacterial infections. Among 278 patients with COVID-19 pneumonia, those treated with antibiotics had more diarrhoea (26, 34.7% vs. 24, 11.8%, < 0.01), while subsequent admissions to the intensive care unit were not lower (6, 8.0% vs. 10, 4.9% = 0.384). Antibiotic treatment was not independently associated with lower 30-day (adjusted odds ratio, aOR 19.528, 95% confidence interval, CI 1.039-367.021) or in-hospital mortality (aOR 3.870, 95% CI 0.433-34.625) rates after adjusting for age, co-morbidities and severity of COVID-19 illness. Compared to white cell count and procalcitonin level, the C-reactive protein level had the best diagnostic accuracy for documented bacterial infections (area under the curve, AUC of 0.822). However, the sensitivity and specificity were less than 90%.
Empiric antibiotic use in those presenting with COVID-19 pneumonia did not prevent deterioration or mortality. More studies are needed to evaluate strategies to diagnose bacterial co-infections in these patients.
由于细菌性肺炎与中度至重度新型冠状病毒肺炎(COVID-19)存在相似性,COVID-19在抗生素决策方面带来了挑战。我们评估了抗生素治疗对COVID-19肺炎患者临床结局的影响以及关键炎症标志物的诊断准确性,以为抗生素决策提供依据。
2020年1月至4月,在新加坡国家传染病中心和樟宜综合医院对因COVID-19住院的患者进行了一项观察性队列研究。如果患者在诊断后3天内开始接受治疗,则被定义为接受了针对COVID-19的经验性抗生素治疗。
在纳入的717例患者中,86例(12.0%)接受了抗生素治疗,26例(3.6%)有记录的细菌感染。在278例COVID-19肺炎患者中,接受抗生素治疗的患者腹泻更多(26例,34.7%对24例,11.8%,<0.01),而随后入住重症监护病房的比例并未降低(6例,8.0%对10例,4.9%,P=0.384)。在调整年龄、合并症和COVID-19疾病严重程度后,抗生素治疗与30天(调整后的优势比,aOR 19.528,95%置信区间,CI 1.039-367.021)或住院死亡率(aOR 3.870,95%CI 0.433-34.625)降低并无独立相关性。与白细胞计数和降钙素原水平相比,C反应蛋白水平对有记录的细菌感染具有最佳诊断准确性(曲线下面积,AUC为0.822)。然而,敏感性和特异性均低于90%。
COVID-19肺炎患者使用经验性抗生素并不能预防病情恶化或死亡。需要更多研究来评估诊断这些患者细菌合并感染的策略。