Kosmala Wojciech, Negishi Tomoko, Thavendiranathan Paaladinesh, Penicka Martin, De Blois Jonathan, Murbræch Klaus, Miyazaki Sakiko, Shirazi Mitra, Santoro Ciro, Vinereanu Dragos, Cho Goo-Yeong, Hristova Krassimira, Popescu Bogdan A, Kurosawa Koji, Izumo Masaki, Negishi Kazuaki, Przewlocka-Kosmala Monika, Marwick Thomas H
Institute of Heart Diseases, Wroclaw Medical University, 50-345 Wroclaw, Poland.
Baker Heart & Diabetes Institute, Melbourne, VIC 3004, Australia.
J Clin Med. 2022 Feb 9;11(4):912. doi: 10.3390/jcm11040912.
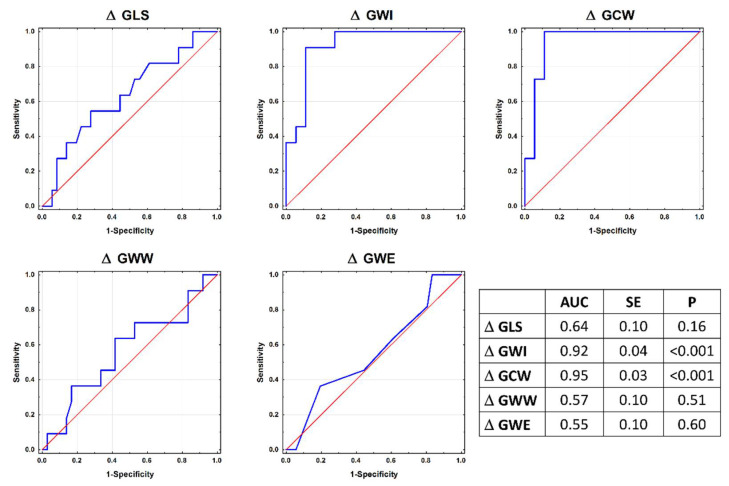
The load dependence of global longitudinal strain (GLS) means that changes in systolic blood pressure (BP) between visits may confound the diagnosis of cancer-treatment-related cardiac dysfunction (CTRCD). We sought to determine whether the estimation of myocardial work, which incorporates SBP, could overcome this limitation. In this case-control study, 44 asymptomatic patients at risk of CTRCD underwent echocardiography at baseline and after oncologic treatment. CTRCD was defined on the basis of the change in the ejection fraction. Those with CTRCD were divided into subsets with and without a follow-up SBP increment >20 mmHg (CTRCD+BP+ and CTRCD+BP-), and matched with patients without CTRCD (CTRCD-BP+ and CTRCD-BP-). The work index (GWI), constructive work (GCW), wasted work (GWW), and work efficiency (GWE) were assessed in addition to the GLS. The largest increases in the GWI and GCW at follow-up were found in CTRCD-BP+ patients. The CTRCD+BP- patients demonstrated significantly larger decreases in GWI and GCW than their CTRCD+BP+ and CTRCD-BP- peers. ROC analysis for the discrimination of LV functional changes in response to increased afterload in the absence of cardiotoxicity revealed higher AUCs for GCW (AUC = 0.97) and GWI (AUC = 0.93) than GLS (AUC = 0.73), GWW (AUC = 0.51), or GWE (AUC = 0.63, all -values < 0.001). GCW (OR: 1.021; 95% CI: 1.001-1.042; < 0.04) was the only feature independently associated with CTRCD-BP+. Myocardial work is superior to GLS in the serial assessments in patients receiving cardiotoxic chemotherapy. The impairment of GLS in the presence of an increase in GWI and GCW indicates the impact of elevated afterload on LV performance in the absence of actual myocardial impairment.
整体纵向应变(GLS)的负荷依赖性意味着就诊期间收缩压(BP)的变化可能会混淆癌症治疗相关心脏功能障碍(CTRCD)的诊断。我们试图确定纳入收缩压的心肌作功评估是否能克服这一局限性。在这项病例对照研究中,44名有CTRCD风险的无症状患者在基线和肿瘤治疗后接受了超声心动图检查。CTRCD根据射血分数的变化来定义。患有CTRCD的患者被分为随访收缩压增量>20 mmHg的亚组和未增量的亚组(CTRCD+BP+和CTRCD+BP-),并与无CTRCD的患者进行匹配(CTRCD-BP+和CTRCD-BP-)。除了GLS外,还评估了作功指数(GWI)、建设性作功(GCW)、浪费作功(GWW)和作功效率(GWE)。随访时GWI和GCW增加最大的是CTRCD-BP+患者。CTRCD+BP-患者的GWI和GCW下降幅度明显大于CTRCD+BP+和CTRCD-BP-的同龄人。在无心脏毒性情况下,用于区分左心室功能随后负荷增加而变化的ROC分析显示,GCW(AUC = 0.97)和GWI(AUC = 0.93)的曲线下面积高于GLS(AUC = 0.73)、GWW(AUC = 0.51)或GWE(AUC = 0.63,所有P值<0.001)。GCW(OR:1.021;95%CI:1.001 - 1.042;P<0.04)是唯一与CTRCD-BP+独立相关的特征。在接受心脏毒性化疗的患者的系列评估中,心肌作功优于GLS。在GWI和GCW增加的情况下GLS受损表明在无实际心肌损伤时后负荷升高对左心室功能的影响。