Center for Clinical Genetics and Genomics, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh Medical Center Magee-Womens Hospital, Pittsburgh, PA.
NRG Oncology, Clinical Trial Development Division, Department of Biostatistics and Bioinformatics, Roswell Park Comprehensive Cancer Center, Buffalo, NY.
Am J Obstet Gynecol. 2022 Jul;227(1):61.e1-61.e18. doi: 10.1016/j.ajog.2022.02.022. Epub 2022 Feb 22.
Risk-reducing salpingo-oophorectomy is an effective ovarian cancer risk reduction strategy. However, bilateral oophorectomy has also been associated with increased long-term nonneoplastic sequelae, effects suggested to be mediated through reductions in systemic sex steroid hormone levels. Currently, it is unclear whether the postmenopausal ovary contributes to the systemic hormonal milieu or whether postmenopausal ovarian volume or other factors, such as body mass index and age, affect systemic hormone levels.
We examined the impact of oophorectomy on sex steroid hormone levels in postmenopausal women. Furthermore, we explored how well ovarian volume measured by transvaginal ultrasound correlated with direct ovarian measures obtained during surgical pathology evaluation and investigated the association between hormone levels and ovarian volumes.
Postmenopausal women who underwent risk-reducing salpingo-oophorectomy (180 cases) or ovarian cancer screening (38 controls) enrolled in an international, prospective study of risk-reducing salpingo-oophorectomy and risk of ovarian cancer algorithm-based screening among women at increased risk of ovarian cancer (Gynecologic Oncology Group-0199) were included in this analysis. Controls were frequency matched to the cases on age at menopause, age at study entry, and time interval between blood draws. Ovarian volume was calculated using measurements obtained from transvaginal ultrasound in both cases and controls and measurements recorded in surgical pathology reports from cases. Serum hormone levels of testosterone, androstenedione, androstenediol, dihydrotestosterone, androsterone, dehydroepiandrosterone, estrone, estradiol, and sex hormone-binding globulin were measured at baseline and follow-up. Spearman correlation coefficients were used to compare ovarian volumes as measured on transvaginal ultrasound and pathology examinations. Correlations between ovarian volumes by transvaginal ultrasound and measured hormone levels were examined using linear regression models. All models were adjusted for age. Paired t tests were performed to evaluate individual differences in hormone levels before and after risk-reducing salpingo-oophorectomy.
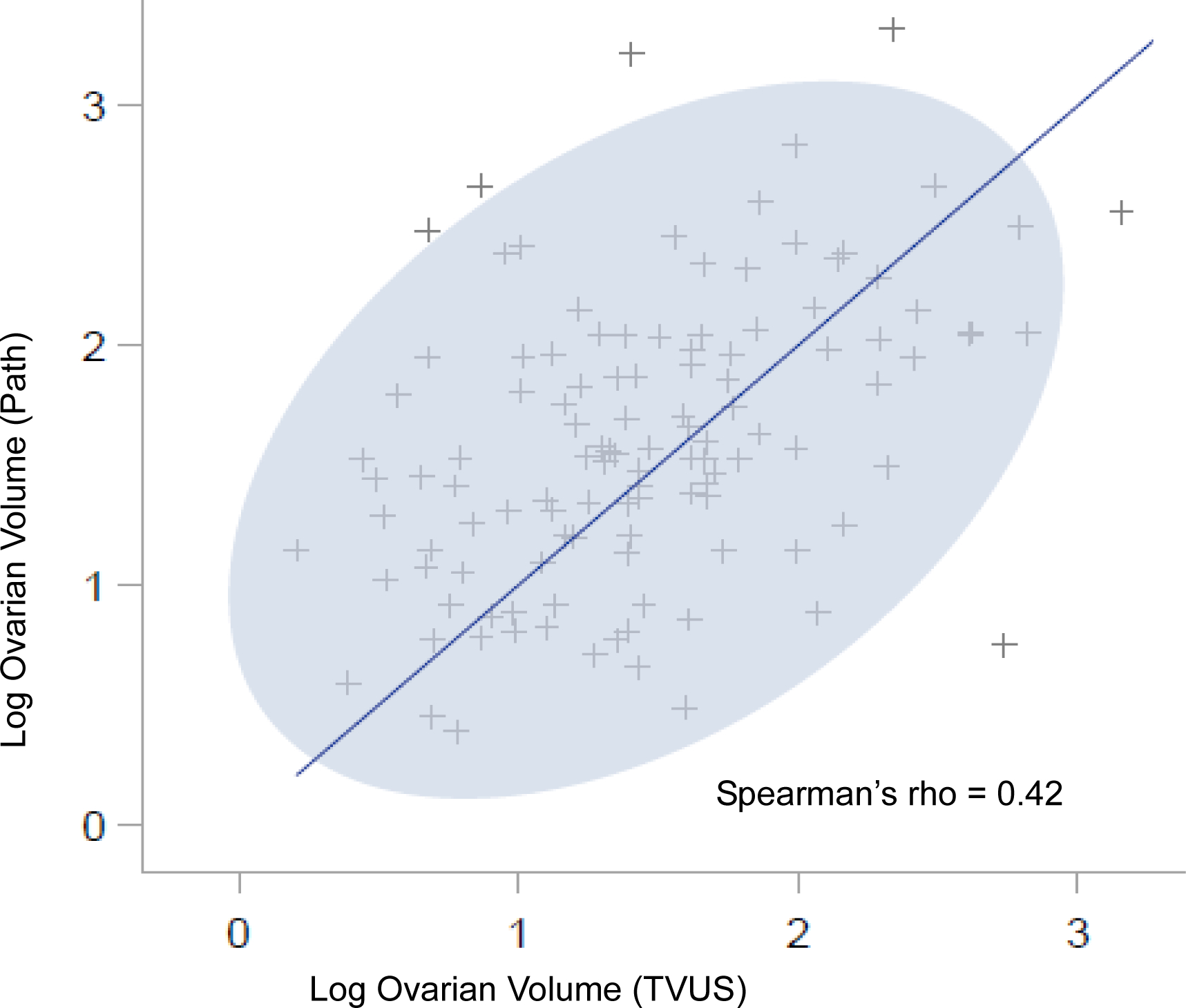
Ovarian volumes measured by transvaginal ultrasound were only moderately correlated with those reported on pathology reports (Spearman rho [ρ]=0.42). The median time interval between risk-reducing salpingo-oophorectomy and follow-up for the cases was 13.3 months (range, 6.0-19.3), and the median time interval between baseline and follow-up for the controls was 12.7 months (range, 8.7-13.4). Sex steroid levels decreased with age but were not correlated with transvaginal ultrasound ovarian volume, body mass index, or time since menopause. Estradiol levels were significantly lower after risk-reducing salpingo-oophorectomy (percentage change, -61.9 post-risk-reducing salpingo-oophorectomy vs +15.2 in controls; P=.02), but no significant differences were seen for the other hormones.
Ovarian volumes measured by transvaginal ultrasound were moderately correlated with volumes directly measured on pathology specimens and were not correlated with sex steroid hormone levels in postmenopausal women. Estradiol was the only hormone that declined significantly after risk-reducing salpingo-oophorectomy. Thus, it remains unclear whether the limited post-risk-reducing salpingo-oophorectomy changes in sex steroid hormones among postmenopausal women impact long-term adverse outcomes.
降低风险的输卵管卵巢切除术是一种有效的卵巢癌风险降低策略。然而,双侧卵巢切除术也与长期非肿瘤性后遗症增加有关,这些影响被认为是通过降低全身性激素水平介导的。目前尚不清楚绝经后卵巢是否有助于全身激素环境,或者绝经后卵巢体积或其他因素(如体重指数和年龄)是否会影响激素水平。
我们研究了卵巢切除术对绝经后妇女性激素水平的影响。此外,我们探讨了经阴道超声测量的卵巢体积与手术病理评估中直接测量的卵巢之间的相关性,并研究了激素水平与卵巢体积之间的关系。
这项分析纳入了参加国际前瞻性降低风险输卵管卵巢切除术和基于卵巢癌风险降低输卵管卵巢切除术和卵巢癌风险算法筛查的研究(妇科肿瘤组-0199)的绝经后妇女,这些妇女接受了降低风险的输卵管卵巢切除术(180 例)或卵巢癌筛查(38 例对照)。对照组按绝经年龄、研究入组时的年龄和采血时间间隔与病例进行频率匹配。病例和对照组均采用经阴道超声测量卵巢体积,并记录手术病理报告中的卵巢体积。基线和随访时测量血清睾酮、雄烯二酮、雄烯二醇、二氢睾酮、雄酮、脱氢表雄酮、雌酮、雌二醇和性激素结合球蛋白的水平。采用 Spearman 相关系数比较经阴道超声和病理检查测量的卵巢体积。采用线性回归模型分析经阴道超声测量的卵巢体积与测量的激素水平之间的相关性。所有模型均按年龄进行调整。采用配对 t 检验评估降低风险的输卵管卵巢切除术前和术后激素水平的个体差异。
经阴道超声测量的卵巢体积与病理报告中报告的卵巢体积仅中度相关(Spearman rho [ρ]=0.42)。病例的中位风险降低输卵管卵巢切除术与随访时间间隔为 13.3 个月(范围,6.0-19.3),对照组的中位基线与随访时间间隔为 12.7 个月(范围,8.7-13.4)。性激素水平随年龄下降,但与经阴道超声卵巢体积、体重指数或绝经后时间无关。与对照组相比(风险降低输卵管卵巢切除术后百分比变化为-61.9%,对照组为+15.2%;P=.02),雌二醇水平在降低风险的输卵管卵巢切除术后显著降低,但其他激素无显著差异。
经阴道超声测量的卵巢体积与病理标本直接测量的体积中度相关,与绝经后妇女的性激素水平无关。雌二醇是唯一在降低风险的输卵管卵巢切除术后明显下降的激素。因此,尚不清楚绝经后妇女降低风险的输卵管卵巢切除术后性激素的有限变化是否会影响长期不良结局。