Department of Neurology, Strasbourg University Hospital, Strasbourg, France.
CHU de Rouen / Rouen University Hospital, 76000, Rouen, France.
J Neuroinflammation. 2022 Mar 2;19(1):62. doi: 10.1186/s12974-022-02420-2.
Neuromyelitis optica spectrum disorder (NMOSD) attacks require an urgent probabilistic anti-inflammatory therapeutic strategy. As inadequately treated attacks result in disability, there is a need to identify the optimal attack-treatment regimen. Our study aimed to identify predictors of outcome after a first attack in patients with an NMOSD presentation and propose the best treatment strategy.
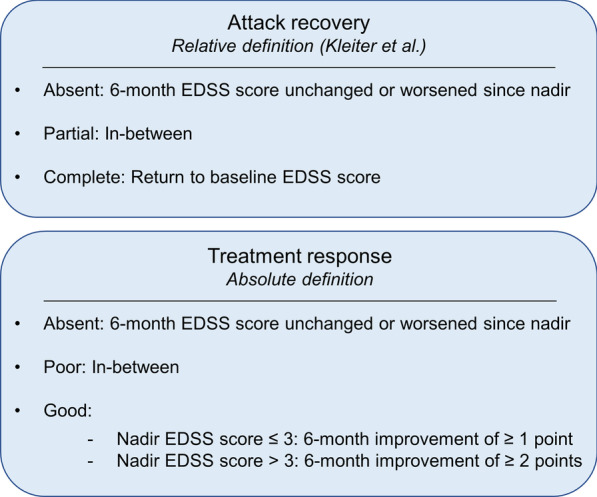
We performed a retrospective cohort study on the French national NMOSD registry (NOMADMUS), a nested cohort of the French multiple sclerosis observatory (OFSEP) recruiting patients with NMOSD presentations in France. We studied the first attack for any independent locations of clinical core characteristic of NMOSD, in treatment-naïve patients. The primary outcome was the evolution of the Expanded Disability Status Scale (EDSS) score at 6 months, stratified in two ways to account for recovery (return to baseline EDSS score) and treatment response (classified as "good" if the EDSS score decreased by ≥ 1 point after a nadir EDSS score ≤ 3, or by ≥ 2 points after a nadir EDSS score > 3). We used ordinal logistic regression to infer statistical associations with the outcome.
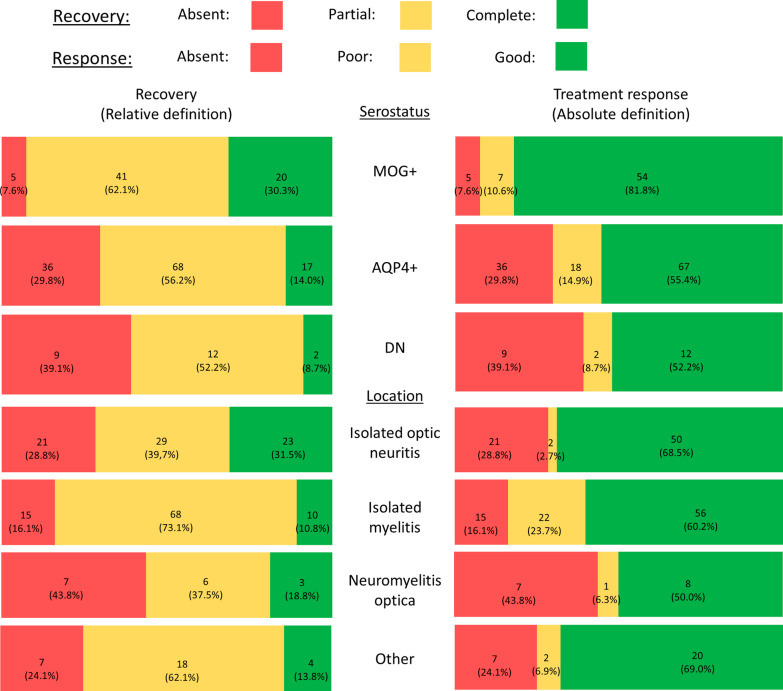
We included 211 attacks among 183 patients (104 with anti-AQP4 antibodies, 60 with anti-MOG antibodies, and 19 double seronegative). Attack treatment regimens comprised corticosteroids (n = 196), plasma exchanges (PE; n = 72) and intravenous immunoglobulins (n = 6). Complete recovery was reached in 40 attacks (19%) at 6 months. The treatment response was "good" in 134 attacks (63.5%). There was no improvement in EDSS score in 50 attacks (23.7%). MOG-antibody seropositivity and short delays to PE were significantly and independently associated with better recovery and treatment response.
We identified two prognostic factors: serostatus (with better outcomes among MOG-Ab-positive patients) and the delay to PE. We, therefore, argue for a more aggressive anti-inflammatory management of the first attacks suggesting an NMOSD presentation, with the early combination of PE with corticosteroids.
视神经脊髓炎谱系疾病(NMOSD)发作需要紧急的概率性抗炎治疗策略。由于治疗不充分的发作导致残疾,因此需要确定最佳的发作治疗方案。我们的研究旨在确定具有 NMOSD 表现的患者首次发作后的结局预测因素,并提出最佳的治疗策略。
我们对法国国家 NMOSD 登记处(NOMADMUS)进行了回顾性队列研究,该登记处是法国多发性硬化症观察站(OFSEP)的一个嵌套队列,招募了法国具有 NMOSD 表现的患者。我们研究了未经治疗的患者中任何独立的 NMOSD 临床核心特征的首发发作。主要结局是 6 个月时扩展残疾状况量表(EDSS)评分的演变,分为两种方式来考虑恢复(恢复到基线 EDSS 评分)和治疗反应(如果 EDSS 评分在最低 EDSS 评分≤3 后下降≥1 点,或在最低 EDSS 评分>3 后下降≥2 点,则被归类为“良好”)。我们使用有序逻辑回归推断与结局的统计学关联。
我们纳入了 183 例患者中的 211 次发作(104 例抗 AQP4 抗体阳性,60 例抗 MOG 抗体阳性,19 例双阴性)。发作治疗方案包括皮质类固醇(n=196)、血浆置换(PE;n=72)和静脉注射免疫球蛋白(n=6)。6 个月时,40 次发作(19%)完全恢复。134 次发作(63.5%)的治疗反应良好。50 次发作(23.7%)的 EDSS 评分无改善。MOG 抗体阳性和 PE 延迟时间较短与更好的恢复和治疗反应显著相关。
我们确定了两个预后因素:血清状态(MOG-Ab 阳性患者的结局更好)和 PE 延迟。因此,我们主张对具有 NMOSD 表现的首次发作进行更积极的抗炎治疗管理,早期联合使用 PE 和皮质类固醇。