Fischer-Valuck Benjamin W, Baumann Brian C, Brown Simon A, Filson Christopher P, Weiss Aaron, Mueller Ryan, Liu Yuan, Brenneman Randall J, Sanda Martin, Michalski Jeff M, Gay Hiram A, James Rao Yuan, Pattaras John G, Jani Ashesh B, Hershatter Bruce, Patel Sagar A
Department of Radiation Oncology, Winship Cancer Institute of Emory University, Atlanta, GA, USA.
Department of Radiation Oncology, Springfield Clinic, Springfield, IL, USA.
Eur Urol Open Sci. 2022 Feb 1;37:80-89. doi: 10.1016/j.euros.2021.12.011. eCollection 2022 Mar.
Elderly patients diagnosed with high-risk prostate cancer (PCa) present a therapeutic dilemma of balancing treatment of a potentially lethal malignancy with overtreatment of a cancer that may not threaten life expectancy.
To investigate treatment patterns and overall survival outcomes in this group of patients.
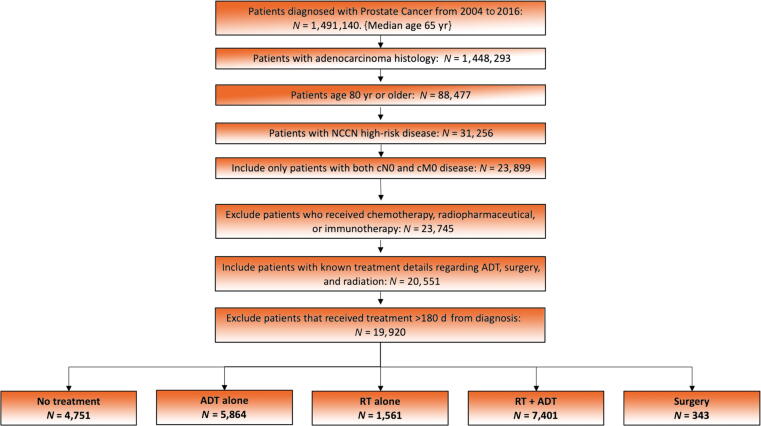
A retrospective cohort study was conducted. We queried the National Cancer Database for high-risk PCa in patients aged 80 yr or older diagnosed during 2004-2016.
Eligible patients underwent no treatment following biopsy (ie, observation), androgen deprivation therapy (ADT) alone, radiation therapy (RT) alone, RT + ADT, or surgery.
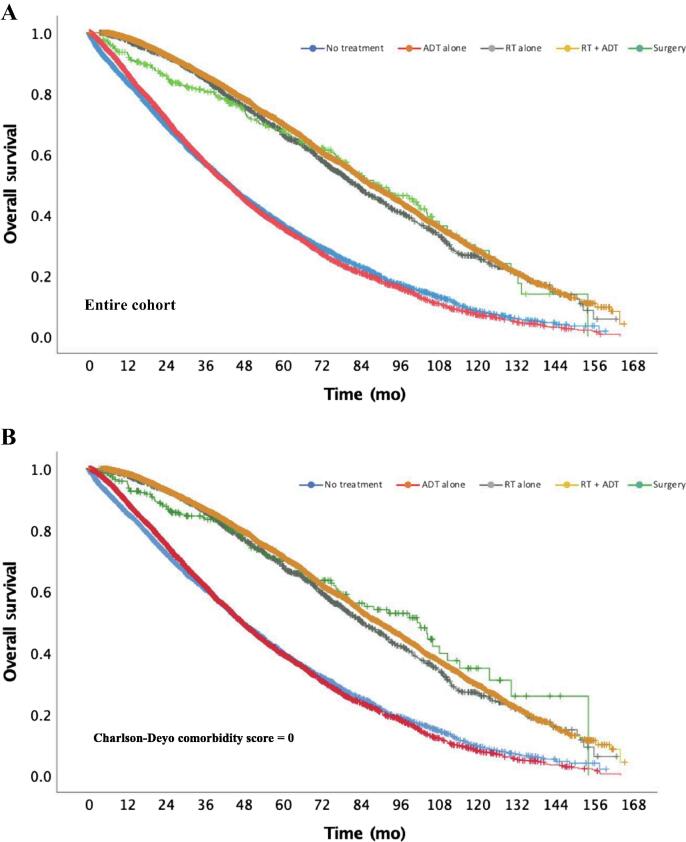
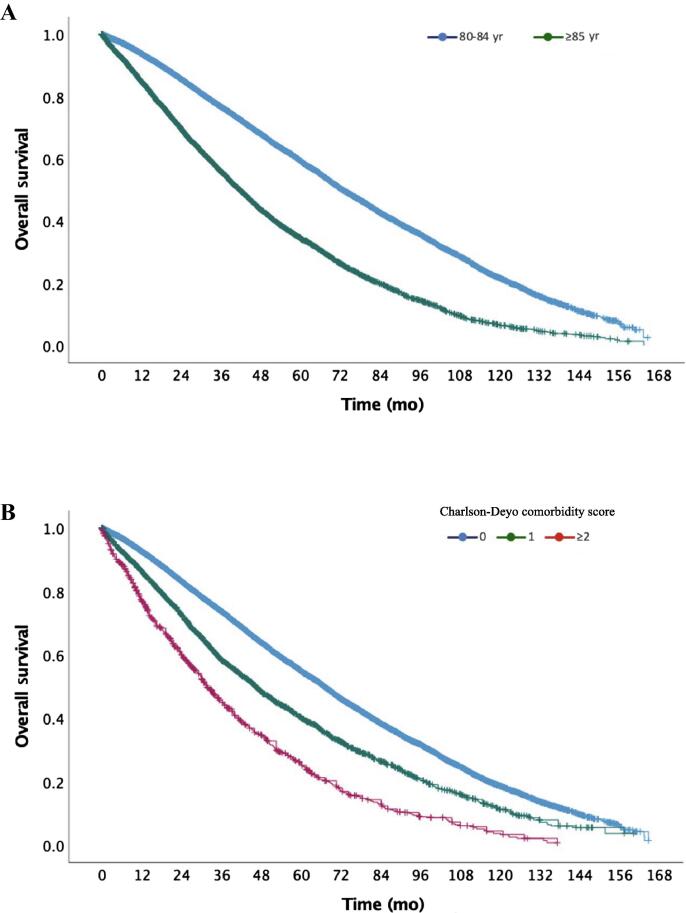
Kaplan-Meier, log rank, and multivariate Cox proportional hazard regression was performed to compare overall survival (OS).
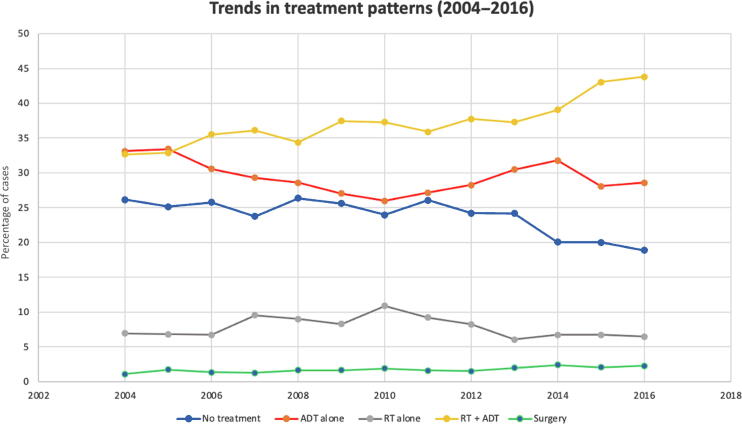
A total of 19 920 men were eligible for analysis, and the most common treatment approach was RT + ADT (7401 patients; 37.2%). Observation and ADT alone declined over time (59.3% in 2004 vs 47.5% in 2016). There was no observed difference in OS between observation and ADT alone (adjusted hazard ratio [HR] 1.04, 95% confidence interval [CI], 0.99-1.09; = 0.105). Definitive local treatment was associated with improved OS compared with ADT alone (RT alone, HR 0.54, 95% CI, 0.50-0.59, < 0.0001; ADT + RT, HR 0.48, 95% CI, 0.46-0.50, < 0.0001; surgery, HR 0.50, 95% CI, 0.42-0.59, < 0.0001).
This analysis demonstrates that the use of definitive local therapy, including surgery or RT ± ADT, is increasing and is associated with a 50% reduction in overall mortality compared with observation or ADT alone. While prospective validation is warranted, elderly men with high-risk disease eligible for definitive management should be counseled on the risks, including a possible compromise in OS, with deferring definitive management.
Elderly men are more often diagnosed with higher-risk prostate cancer but are less likely to receive curative treatment options than younger men. Our analysis demonstrates that for men ≥80 yr of age with high-risk prostate cancer, definitive local therapy, including surgery or radiation therapy and/or androgen deprivation therapy, is associated with a 50% reduction in overall mortality compared with observation or androgen deprivation therapy alone. We therefore recommend that life expectancy (ie, physiologic age) be taken into account, over chronologic age, and that elderly men with good life expectancy (eg, >5 yr; minimal comorbidity) should be offered definitive, life-prolonging therapy.
被诊断为高危前列腺癌(PCa)的老年患者面临着一种治疗困境,即如何在治疗可能致命的恶性肿瘤与过度治疗可能不影响预期寿命的癌症之间取得平衡。
研究该组患者的治疗模式和总生存结果。
设计、设置与参与者:进行了一项回顾性队列研究。我们查询了国家癌症数据库中2004 - 2016年期间诊断为高危PCa的80岁及以上患者的数据。
符合条件的患者在活检后未接受任何治疗(即观察)、仅接受雄激素剥夺治疗(ADT)、仅接受放射治疗(RT)、RT + ADT或手术。
采用Kaplan - Meier法、对数秩检验和多变量Cox比例风险回归分析来比较总生存期(OS)。
共有19920名男性符合分析条件,最常见的治疗方法是RT + ADT(7401例患者;37.2%)。观察和仅ADT治疗的比例随时间下降(2004年为59.3%,2016年为47.5%)。观察和仅ADT治疗之间的OS未观察到差异(调整后风险比[HR]为1.04,95%置信区间[CI]为0.99 - 1.09;P = 0.105)。与仅ADT治疗相比,确定性局部治疗与改善的OS相关(仅RT治疗,HR为0.54,95% CI为0.50 - 0.59,P < 0.0001;ADT + RT治疗,HR为0.48,95% CI为0.46 - 0.50,P < 0.0001;手术治疗,HR为0.50,95% CI为0.42 - 0.59,P < 0.0001)。
该分析表明,包括手术或RT ± ADT在内的确定性局部治疗的使用正在增加,与仅观察或仅ADT治疗相比,总死亡率降低了50%。虽然需要进行前瞻性验证,但对于适合确定性治疗的高危老年男性,应就推迟确定性治疗的风险(包括可能影响OS)进行咨询。
老年男性更常被诊断为高危前列腺癌,但与年轻男性相比,接受根治性治疗的可能性较小。我们的分析表明,对于80岁及以上的高危前列腺癌男性,与仅观察或仅雄激素剥夺治疗相比,包括手术或放射治疗和/或雄激素剥夺治疗在内的确定性局部治疗可使总死亡率降低50%。因此,我们建议应考虑预期寿命(即生理年龄)而非实际年龄,对于预期寿命良好(例如,>5年;合并症极少)的老年男性,应提供确定性的延长生命治疗。