BMC Med. 2022 Mar 7;20(1):85. doi: 10.1186/s12916-022-02265-9.
Plasmodium falciparum malaria is associated with anaemia-related morbidity, attributable to host, parasite and drug factors. We quantified the haematological response following treatment of uncomplicated P. falciparum malaria to identify the factors associated with malarial anaemia.
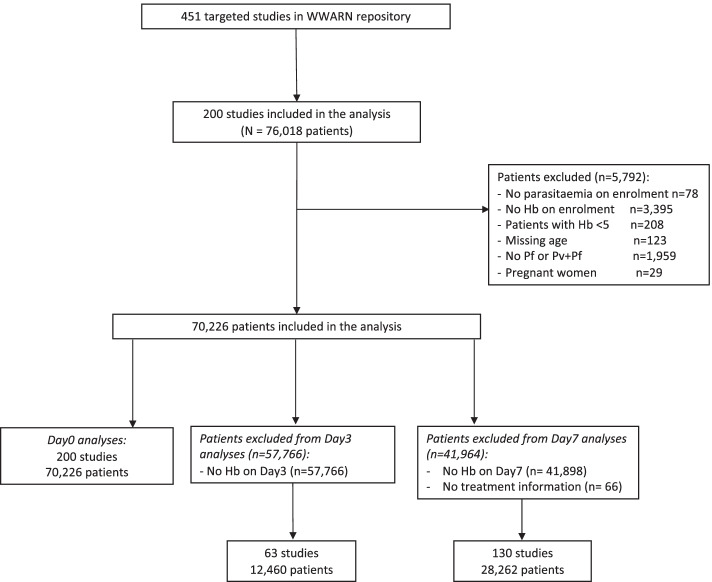
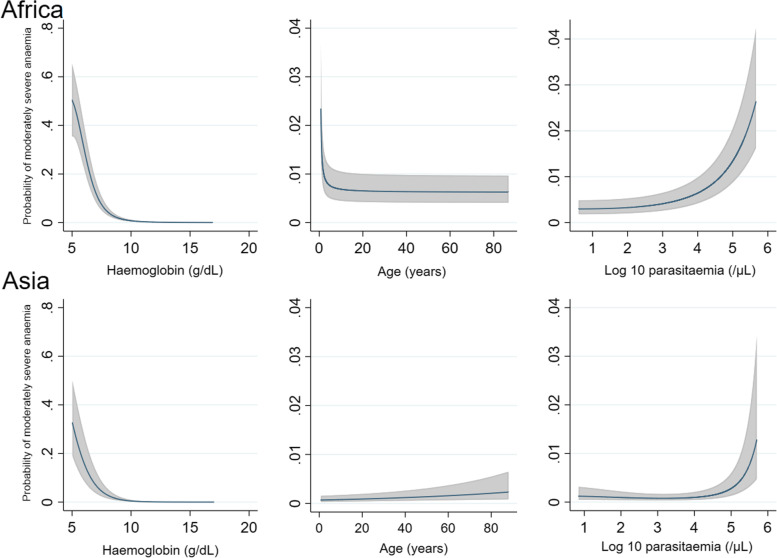
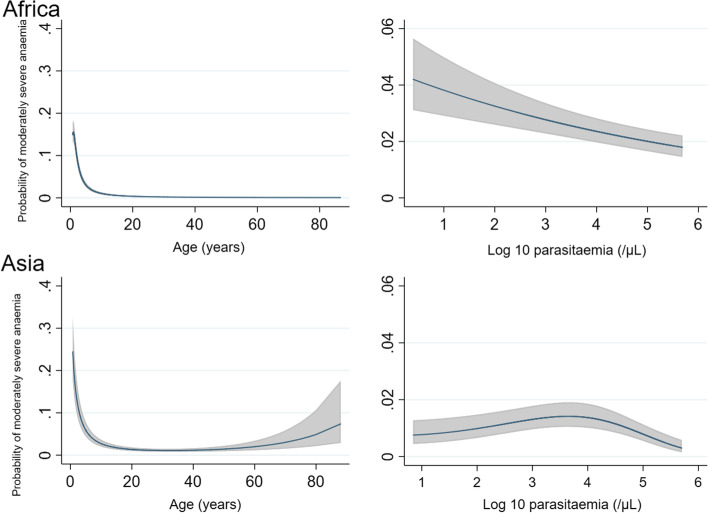
Individual patient data from eligible antimalarial efficacy studies of uncomplicated P. falciparum malaria, available through the WorldWide Antimalarial Resistance Network data repository prior to August 2015, were pooled using standardised methodology. The haematological response over time was quantified using a multivariable linear mixed effects model with nonlinear terms for time, and the model was then used to estimate the mean haemoglobin at day of nadir and day 7. Multivariable logistic regression quantified risk factors for moderately severe anaemia (haemoglobin < 7 g/dL) at day 0, day 3 and day 7 as well as a fractional fall ≥ 25% at day 3 and day 7.
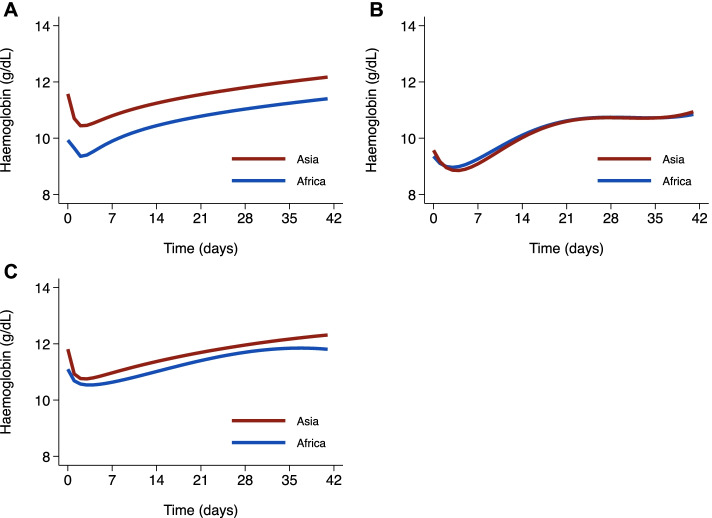
A total of 70,226 patients, recruited into 200 studies between 1991 and 2013, were included in the analysis: 50,859 (72.4%) enrolled in Africa, 18,451 (26.3%) in Asia and 916 (1.3%) in South America. The median haemoglobin concentration at presentation was 9.9 g/dL (range 5.0-19.7 g/dL) in Africa, 11.6 g/dL (range 5.0-20.0 g/dL) in Asia and 12.3 g/dL (range 6.9-17.9 g/dL) in South America. Moderately severe anaemia (Hb < 7g/dl) was present in 8.4% (4284/50,859) of patients from Africa, 3.3% (606/18,451) from Asia and 0.1% (1/916) from South America. The nadir haemoglobin occurred on day 2 post treatment with a mean fall from baseline of 0.57 g/dL in Africa and 1.13 g/dL in Asia. Independent risk factors for moderately severe anaemia on day 7, in both Africa and Asia, included moderately severe anaemia at baseline (adjusted odds ratio (AOR) = 16.10 and AOR = 23.00, respectively), young age (age < 1 compared to ≥ 12 years AOR = 12.81 and AOR = 6.79, respectively), high parasitaemia (AOR = 1.78 and AOR = 1.58, respectively) and delayed parasite clearance (AOR = 2.44 and AOR = 2.59, respectively). In Asia, patients treated with an artemisinin-based regimen were at significantly greater risk of moderately severe anaemia on day 7 compared to those treated with a non-artemisinin-based regimen (AOR = 2.06 [95%CI 1.39-3.05], p < 0.001).
In patients with uncomplicated P. falciparum malaria, the nadir haemoglobin occurs 2 days after starting treatment. Although artemisinin-based treatments increase the rate of parasite clearance, in Asia they are associated with a greater risk of anaemia during recovery.
恶性疟原虫疟疾与贫血相关的发病率有关,这归因于宿主、寄生虫和药物因素。我们量化了治疗无并发症恶性疟原虫疟疾后的血液学反应,以确定与疟疾性贫血相关的因素。
在 2015 年 8 月之前,通过世界疟疾抗药性网络数据存储库,汇集了无并发症恶性疟原虫疟疾的合格抗疟疗效研究的个体患者数据,使用标准化方法进行处理。使用具有非线性时间项的多变量线性混合效应模型来量化随时间的血液学反应,然后使用该模型估计第 0 天、第 7 天的最低血红蛋白值和第 7 天的平均血红蛋白值。多变量逻辑回归量化了第 0 天、第 3 天和第 7 天中度严重贫血(血红蛋白 <7g/dL)以及第 3 天和第 7 天血红蛋白下降≥25%的风险因素。
共纳入 70226 名患者,这些患者分别在 1991 年至 2013 年期间参与了 200 项研究:50859 名(72.4%)在非洲招募,18451 名(26.3%)在亚洲招募,916 名(1.3%)在南美洲招募。在非洲,就诊时的中位血红蛋白浓度为 9.9g/dL(范围 5.0-19.7g/dL),亚洲为 11.6g/dL(范围 5.0-20.0g/dL),南美洲为 12.3g/dL(范围 6.9-17.9g/dL)。在非洲,4284/50859(8.4%)的患者出现中度严重贫血(Hb<7g/dl),亚洲为 606/18451(3.3%),南美洲为 1/916(0.1%)。治疗后第 2 天出现最低血红蛋白值,与基线相比,非洲平均下降 0.57g/dL,亚洲下降 1.13g/dL。在非洲和亚洲,第 7 天出现中度严重贫血的独立风险因素包括基线时中度严重贫血(调整后的优势比(AOR)分别为 16.10 和 AOR = 23.00)、年龄较小(年龄 <1 与年龄≥12 岁相比,AOR = 12.81 和 AOR = 6.79)、高寄生虫血症(AOR = 1.78 和 AOR = 1.58)和寄生虫清除延迟(AOR = 2.44 和 AOR = 2.59)。在亚洲,与使用非青蒿素类药物治疗的患者相比,使用青蒿素类药物治疗的患者在第 7 天出现中度严重贫血的风险显著增加(AOR = 2.06[95%CI 1.39-3.05],p<0.001)。
在患有无并发症恶性疟原虫疟疾的患者中,血红蛋白最低值发生在开始治疗后的第 2 天。尽管青蒿素类药物治疗可提高寄生虫清除率,但在亚洲,它们与恢复期贫血风险增加有关。