Division of Nephrology, Department of Medicine, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Canada.
Ontario Renal Network, Ontario Health, Toronto, Canada.
J Am Soc Nephrol. 2022 Apr;33(4):839-849. doi: 10.1681/ASN.2021091262. Epub 2022 Mar 9.
Vaccination studies in the hemodialysis population have demonstrated decreased antibody response compared with healthy controls, but vaccine effectiveness for preventing SARS-CoV-2 infection and severe disease is undetermined.
We conducted a retrospective cohort study in the province of Ontario, Canada, between December 21, 2020, and June 30, 2021. Receipt of vaccine, SARS-CoV-2 infection, and related severe outcomes (hospitalization or death) were determined from provincial health administrative data. Receipt of one and two doses of vaccine were modeled in a time-varying cause-specific Cox proportional hazards model, adjusting for baseline characteristics, background community infection rates, and censoring for non-COVID death, recovered kidney function, transfer out of province, solid organ transplant, and withdrawal from dialysis.
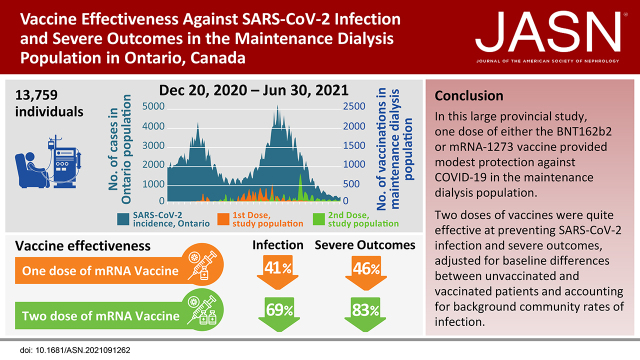
Among 13,759 individuals receiving maintenance dialysis, 2403 (17%) were unvaccinated and 11,356 (83%) had received at least one dose by June 30, 2021. Vaccine types were BNT162b2 (=8455, 74%) and mRNA-1273 (=2901, 26%); median time between the first and second dose was 36 days (IQR 28-51). The adjusted hazard ratio (HR) for SARS-CoV-2 infection and severe outcomes for one dose compared with unvaccinated was 0.59 (95% CI, 0.46 to 0.76) and 0.54 (95% CI, 0.37 to 0.77), respectively, and for two doses compared with unvaccinated was 0.31 (95% CI, 0.22 to 0.42) and 0.17 (95% CI, 0.1 to 0.3), respectively. There were no significant differences in vaccine effectiveness among age groups, dialysis modality, or vaccine type.
COVID-19 vaccination is effective in the dialysis population to prevent SARS-CoV-2 infection and severe outcomes, despite concerns about suboptimal antibody responses.
与健康对照相比,血液透析人群中的疫苗接种研究表明抗体反应降低,但疫苗预防 SARS-CoV-2 感染和严重疾病的有效性尚不确定。
我们在加拿大安大略省进行了一项回顾性队列研究,时间为 2020 年 12 月 21 日至 2021 年 6 月 30 日。从省级卫生行政数据中确定疫苗接种、SARS-CoV-2 感染和相关严重结局(住院或死亡)。使用时变特定原因 Cox 比例风险模型对一剂和两剂疫苗接种进行建模,调整了基线特征、背景社区感染率以及非 COVID 死亡、恢复的肾功能、转出省、实体器官移植和退出透析的截止时间。
在 13759 名接受维持性透析的患者中,2403 名(17%)未接种疫苗,11356 名(83%)在 2021 年 6 月 30 日前至少接种了一剂疫苗。疫苗类型为 BNT162b2(=8455,74%)和 mRNA-1273(=2901,26%);第一剂和第二剂之间的中位时间为 36 天(IQR 28-51)。与未接种疫苗相比,一剂疫苗的 SARS-CoV-2 感染和严重结局的调整后危险比(HR)分别为 0.59(95%CI,0.46 至 0.76)和 0.54(95%CI,0.37 至 0.77),两剂疫苗分别为 0.31(95%CI,0.22 至 0.42)和 0.17(95%CI,0.1 至 0.3)。在年龄组、透析方式或疫苗类型方面,疫苗有效性没有显著差异。
尽管对抗体反应不理想存在担忧,但 COVID-19 疫苗在透析人群中可有效预防 SARS-CoV-2 感染和严重结局。