Trommer Maike, Adams Anne, Celik Eren, Fan Jiaqi, Funken Dominik, Herter Jan M, Linde Philipp, Morgenthaler Janis, Wegen Simone, Mauch Cornelia, Franklin Cindy, Galldiks Norbert, Werner Jan-Michael, Kocher Martin, Rueß Daniel, Ruge Maximilian, Meißner Anna-Katharina, Baues Christian, Marnitz Simone
Department of Radiation Oncology, Cyberknife Center, Faculty of Medicine, University Hospital Cologne, University of Cologne, 50937 Cologne, Germany.
Center of Integrated Oncology (CIO), Universities of Aachen, Bonn, Cologne, and Düsseldorf, 50937 Cologne, Germany.
Cancers (Basel). 2022 Feb 27;14(5):1240. doi: 10.3390/cancers14051240.
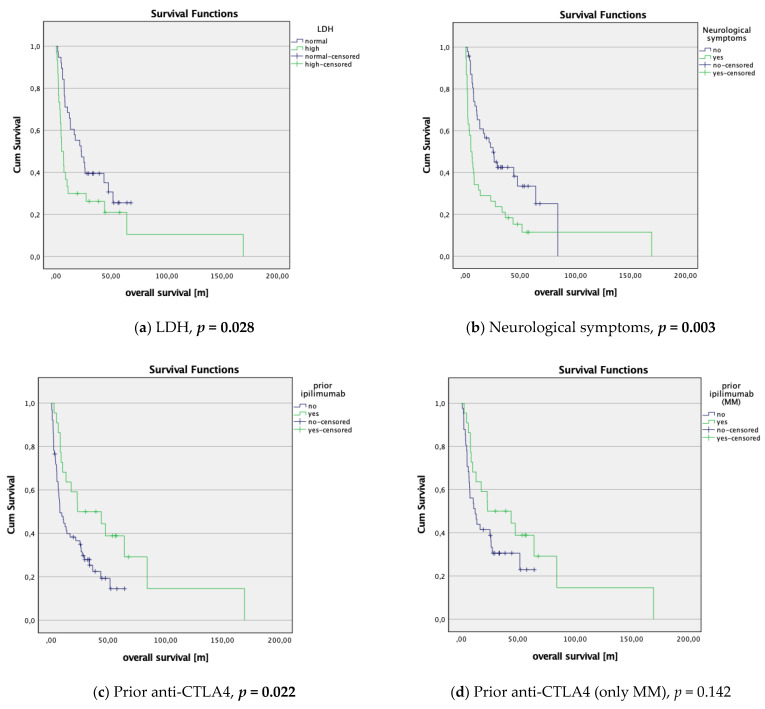
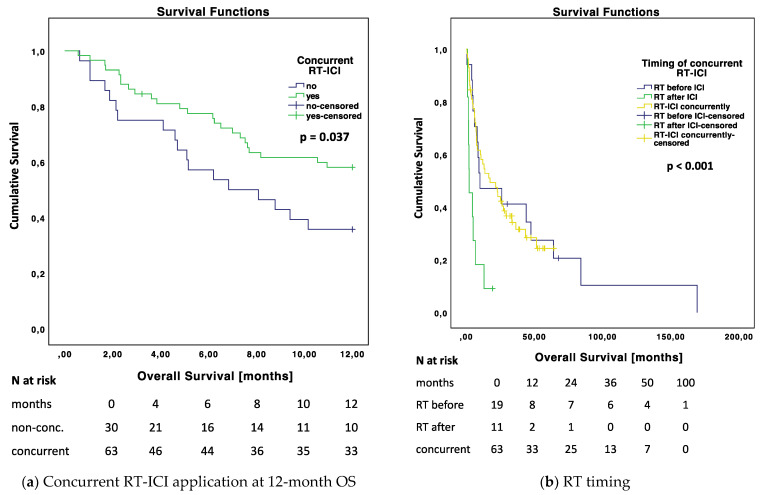
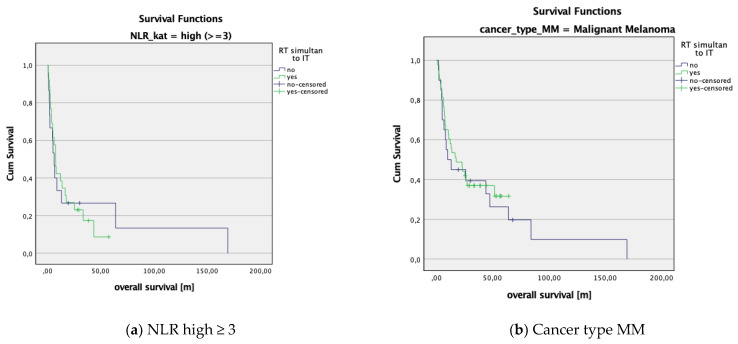
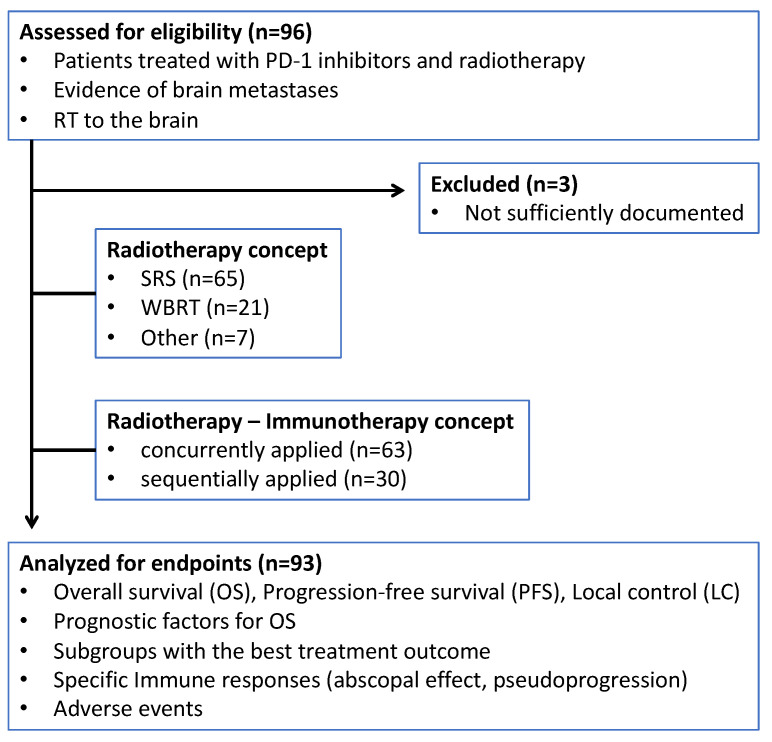
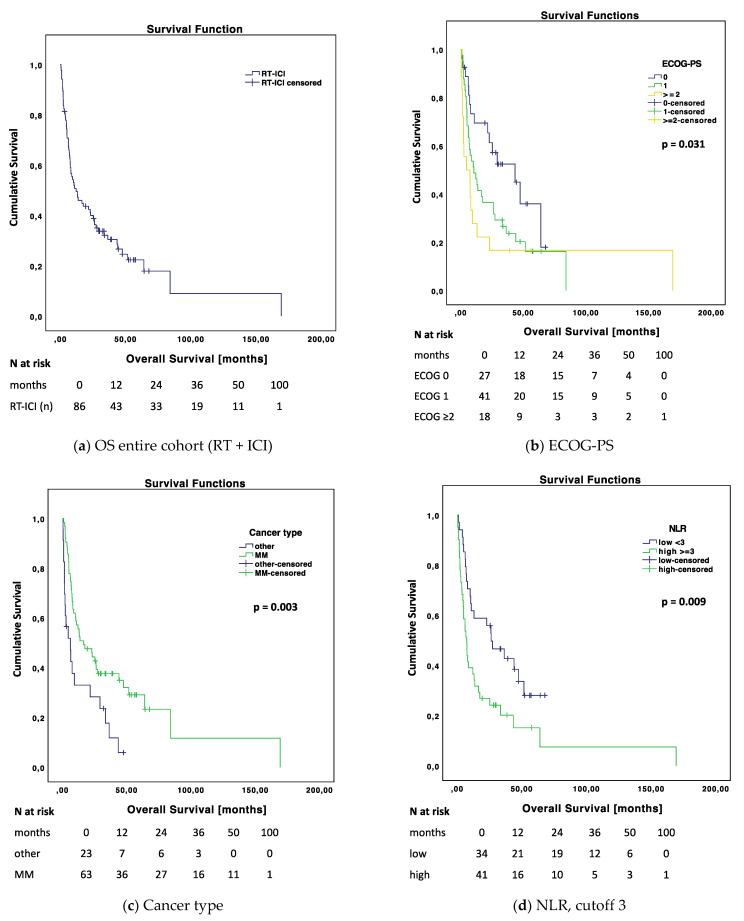
While immune checkpoint inhibitors (ICIs) in combination with radiotherapy (RT) are widely used for patients with brain metastasis (BM), markers that predict treatment response for combined RT and ICI (RT-ICI) and their optimal dosing and sequence for the best immunogenic effects are still under investigation. The aim of this study was to evaluate prognostic factors for therapeutic outcome and to compare effects of concurrent and non-concurrent RT-ICI. We retrospectively analyzed data of 93 patients with 319 BMs of different cancer types who received PD-1 inhibitors and RT at the University Hospital Cologne between September/2014 and November/2020. Primary study endpoints were overall survival (OS), progression-free survival (PFS), and local control (LC). We included 66.7% melanoma, 22.8% lung, and 5.5% other cancer types with a mean follow-up time of 23.8 months. Median OS time was 12.19 months. LC at 6 months was 95.3% (concurrent) vs. 69.2% (non-concurrent; p = 0.008). Univariate Cox regression analysis detected following prognostic factors for OS: neutrophil-to-lymphocyte ratio NLR favoring <3 (low; HR 2.037 (1.184−3.506), p = 0.010), lactate dehydrogenase (LDH) favoring ≤ULN (HR 1.853 (1.059−3.241), p = 0.031), absence of neurological symptoms (HR 2.114 (1.285−3.478), p = 0.003), RT concept favoring SRS (HR 1.985 (1.112−3.543), p = 0.019), RT dose favoring ≥60 Gy (HR 0.519 (0.309−0.871), p = 0.013), and prior anti-CTLA4 treatment (HR 0.498 (0.271−0.914), p = 0.024). Independent prognostic factors for OS were concurrent RT-ICI application (HR 0.539 (0.299−0.971), p = 0.024) with a median OS of 17.61 vs. 6.83 months (non-concurrent), ECOG performance status favoring 0 (HR 7.756 (1.253−6.061), p = 0.012), cancer type favoring melanoma (HR 0.516 (0.288−0.926), p = 0.026), BM volume (PTV) favoring ≤3 cm3 (HR 1.947 (1.007−3.763), p = 0.048). Subgroups with the following factors showed significantly longer OS when being treated concurrently: RT dose <60 Gy (p = 0.014), PTV > 3 cm3 (p = 0.007), other cancer types than melanoma (p = 0.006), anti-CTLA4-naïve patients (p < 0.001), low NLR (p = 0.039), steroid intake ≤4 mg (p = 0.042). Specific immune responses, such as abscopal effects (AbEs), pseudoprogression (PsP), or immune-related adverse events (IrAEs), occurred more frequently with concurrent RT-ICI and resulted in better OS. Other toxicities, including radionecrosis, were not statistically different in both groups. The concurrent application of RT and ICI, the ECOG-PS, cancer type, and PTV had an independently prognostic impact on OS. In concurrently treated patients, treatment response (LC) was delayed and specific immune responses (AbE, PsP, IrAE) occurred more frequently with longer OS rates. Our results suggest that concurrent RT-ICI application is more beneficial than sequential treatment in patients with low pretreatment inflammatory status, more and larger BMs, and with other cancer types than melanoma.
虽然免疫检查点抑制剂(ICI)联合放射治疗(RT)广泛应用于脑转移(BM)患者,但预测联合放疗和ICI(RT-ICI)治疗反应的标志物及其产生最佳免疫原性效应的最佳剂量和顺序仍在研究中。本研究的目的是评估治疗结果的预后因素,并比较同步和非同步RT-ICI的效果。我们回顾性分析了2014年9月至2020年11月在科隆大学医院接受PD-1抑制剂和放疗的93例不同癌症类型的319个脑转移患者的数据。主要研究终点为总生存期(OS)、无进展生存期(PFS)和局部控制(LC)。我们纳入了66.7%的黑色素瘤、22.8%的肺癌和5.5%的其他癌症类型,平均随访时间为23.8个月。中位OS时间为12.19个月。6个月时的LC为95.3%(同步)对69.2%(非同步;p = 0.008)。单因素Cox回归分析检测到以下OS的预后因素:中性粒细胞与淋巴细胞比值NLR <3(低;HR 2.037(1.184−3.506),p = 0.010),乳酸脱氢酶(LDH)≤ULN(HR 1.853(1.059−3.241),p = 0.031),无神经症状(HR 2.114(1.285−3.478),p = 0.003),放疗方案倾向于立体定向放射治疗(SRS)(HR 1.985(1.112−3.543),p = 0.019),放疗剂量≥60 Gy(HR 0.519(0.309−0.871),p = 0.013),以及既往抗CTLA4治疗(HR 0.498(0.271−0.914),p = 0.024)。OS的独立预后因素为同步应用RT-ICI(HR = 0.539(0.299−0.971),p = 0.024),中位OS为17.61个月对6.83个月(非同步),ECOG体能状态为0(HR 7.756(1.253−6.061),p = 0.012),癌症类型为黑色素瘤(HR 0.516(0.288−0.926),p = 0.026),脑转移瘤体积(PTV)≤3 cm3(HR 1.947(1.007−3.763),p = 0.048)!具有以下因素的亚组在同步治疗时显示出显著更长的OS:放疗剂量<60 Gy(p = 0.014),PTV>3 cm3(p = 0.007),非黑色素瘤的其他癌症类型(p = 0.006),未使用过抗CTLA4的患者(p < 0.001),低NLR(p = 0.039),类固醇摄入量≤4 mg(p = 0.042)。特定的免疫反应,如远隔效应(AbE)、假性进展(PsP)或免疫相关不良事件(IrAE),在同步RT-ICI治疗时更频繁发生,并导致更好的OS。包括放射性坏死在内的其他毒性在两组中无统计学差异。RT和ICI的同步应用、ECOG-PS、癌症类型和PTV对OS有独立的预后影响。在同步治疗的患者中,治疗反应(LC)延迟,特定免疫反应(AbE、PsP、IrAE)更频繁发生,OS率更长。我们的结果表明,对于预处理炎症状态低、脑转移瘤数量多且体积大、非黑色素瘤的其他癌症类型的患者,同步应用RT-ICI比序贯治疗更有益。