Na Soo Jin, Youn Jong-Chan, Lee Hye Sun, Jeon Soyoung, Lee Hae-Young, Cho Hyun-Jai, Choi Jin-Oh, Jeon Eun-Seok, Lee Sang Eun, Kim Min-Seok, Kim Jae-Joong, Hwang Kyung-Kuk, Cho Myeong-Chan, Chae Shung Chull, Kang Seok-Min, Choi Dong-Ju, Yoo Byung-Su, Kim Kye Hoon, Oh Byung-Hee, Baek Sang Hong
Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, South Korea.
Department of Medicine, Catholic University Graduate School, Seoul, South Korea.
Front Cardiovasc Med. 2022 Feb 22;9:791446. doi: 10.3389/fcvm.2022.791446. eCollection 2022.
Randomized clinical trials of spironolactone showed significant mortality reduction in patients with heart failure with reduced ejection fraction. However, its role in acute heart failure syndrome (AHFS) is largely unknown.
To investigate the prescription characteristics, efficacy and safety of spironolactone in real-world patients with AHFS.
5,136 AHFS patients who survived to hospital discharge using a nationwide prospective registry in Korea were analyzed. The primary efficacy outcome was 3-year all-cause mortality.
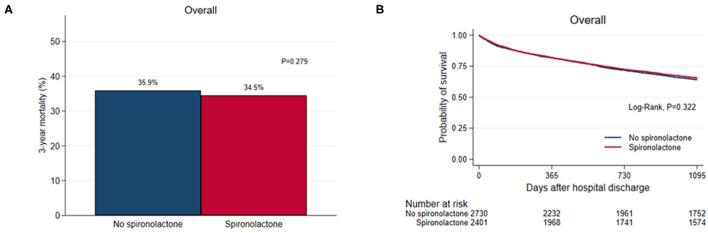
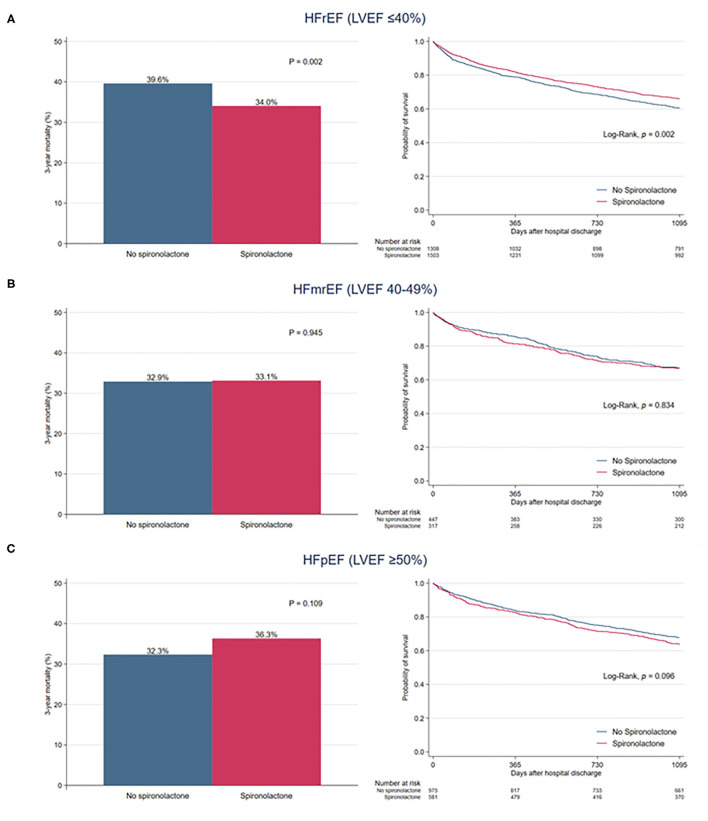
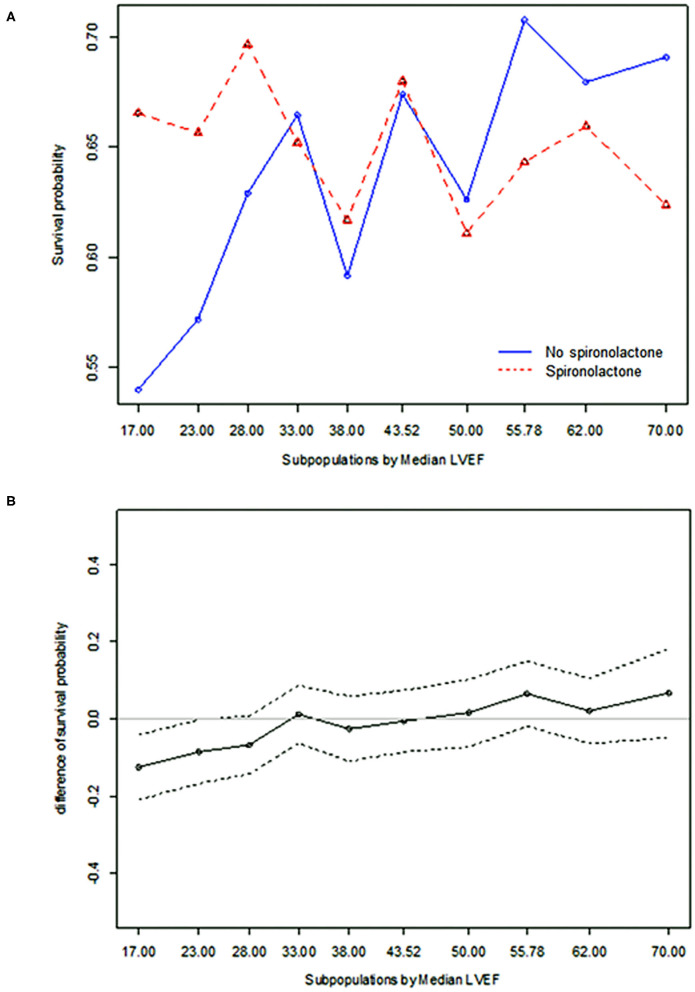
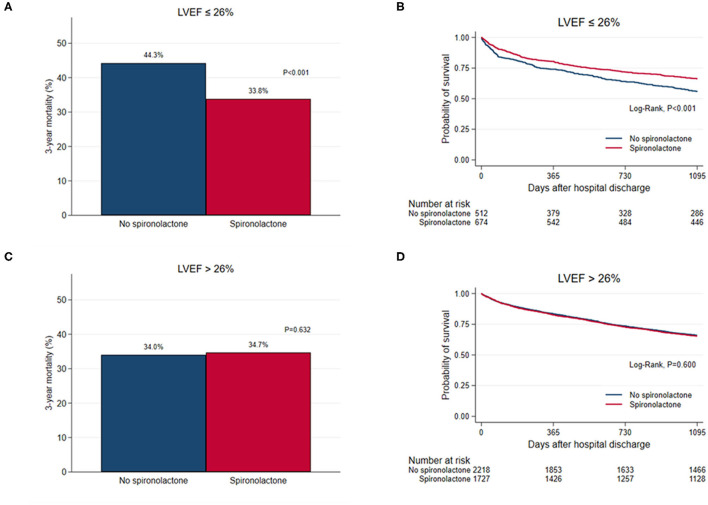
Spironolactone was prescribed in 2,402 (46.8%) at discharge: <25 mg in 890 patients (37.1%), ≥25 mg, and <50 mg in 1,154 patients (48.0%), and ≥50 mg in 358 patients (14.9%). Patients treated with spironolactone had a lower proportion of chronic renal failure and renal replacement therapy during hospitalization and had lower serum creatinine level than those who did not. In overall patients, 3-year mortality was not different in both groups (35.9 vs. 34.5%, = 0.279). The incidence of renal injury and hyperkalemia was 2.2% and 4.3%, respectively, at the first follow-up visit. The treatment effect of spironolactone on mortality was different across subpopulations according to LVEF. The use of spironolactone was associated with a significant reduction in 3-year morality in patients with LVEF ≤ 26% (33.8 vs. 44.3%, < 0.001; adjusted HR 0.79, 95% CI 0.64-0.97, = 0.023), but not in patients with LVEF > 26%.
Although spironolactone was frequently used at lower doses in real-world practice, use of spironolactone significantly reduced 3-year mortality in patients with severely reduced LVEF with acceptable safety profile. However, our findings remain prone to various biases and further prospective randomized controlled studies are needed to confirm these findings.
螺内酯的随机临床试验表明,射血分数降低的心力衰竭患者的死亡率显著降低。然而,其在急性心力衰竭综合征(AHFS)中的作用在很大程度上尚不清楚。
研究螺内酯在现实世界中AHFS患者中的处方特征、疗效和安全性。
对韩国一项全国性前瞻性登记中存活至出院的5136例AHFS患者进行分析。主要疗效结局为3年全因死亡率。
出院时2402例(46.8%)患者使用了螺内酯:890例患者(37.1%)剂量<25mg,1154例患者(48.0%)剂量≥25mg且<50mg,358例患者(14.9%)剂量≥50mg。与未使用螺内酯的患者相比,使用螺内酯治疗的患者住院期间慢性肾衰竭和肾脏替代治疗的比例较低,血清肌酐水平也较低。在所有患者中,两组的3年死亡率无差异(35.9%对34.5%,P=0.279)。首次随访时,肾损伤和高钾血症的发生率分别为2.2%和4.3%。根据左心室射血分数(LVEF),螺内酯对不同亚组患者死亡率的治疗效果不同。LVEF≤ 26% 的患者使用螺内酯与3年死亡率显著降低相关(33.8%对44.3%,P<0.001;调整后风险比0.79,95%可信区间0.64-0.97,P=0.023),但LVEF>26%的患者并非如此。
虽然在现实世界的实践中,螺内酯经常以较低剂量使用,但对于LVEF严重降低的患者,使用螺内酯可显著降低3年死亡率,且安全性可接受。然而,我们的研究结果仍容易受到各种偏倚的影响,需要进一步的前瞻性随机对照研究来证实这些发现。