Muse Evan D, Chen Shang-Fu, Liu Shuchen, Fernandez Brianna, Schrader Brian, Molparia Bhuvan, León André Nicolás, Lee Raymond, Pubbi Neha, Mejia Nolan, Ren Christina, El-Kalliny Ahmed, Prado Montes de Oca Ernesto, Aguilar Hector, Ghoshal Arjun, Dias Raquel, Evans Doug, Chen Kai-Yu, Zhang Yunyue, Wineinger Nathan E, Spencer Emily G, Topol Eric J, Torkamani Ali
Scripps Research Translational Institute, La Jolla, CA, 92037, USA.
Scripps Clinic, La Jolla, CA, 92037, USA.
NPJ Digit Med. 2022 Mar 11;5(1):30. doi: 10.1038/s41746-022-00578-w.
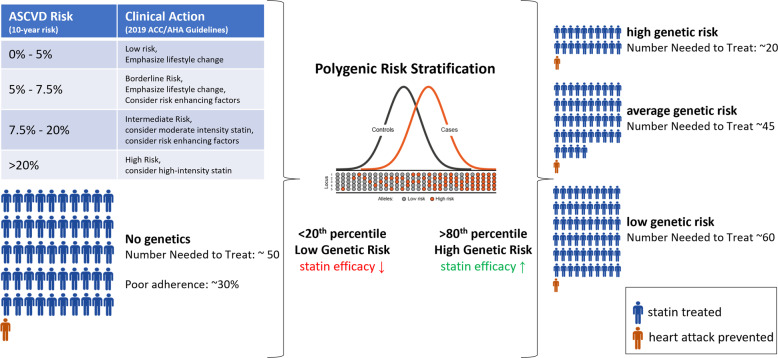
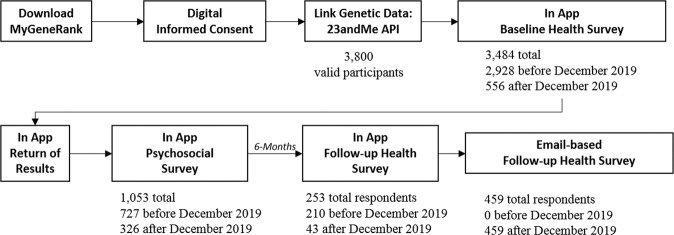
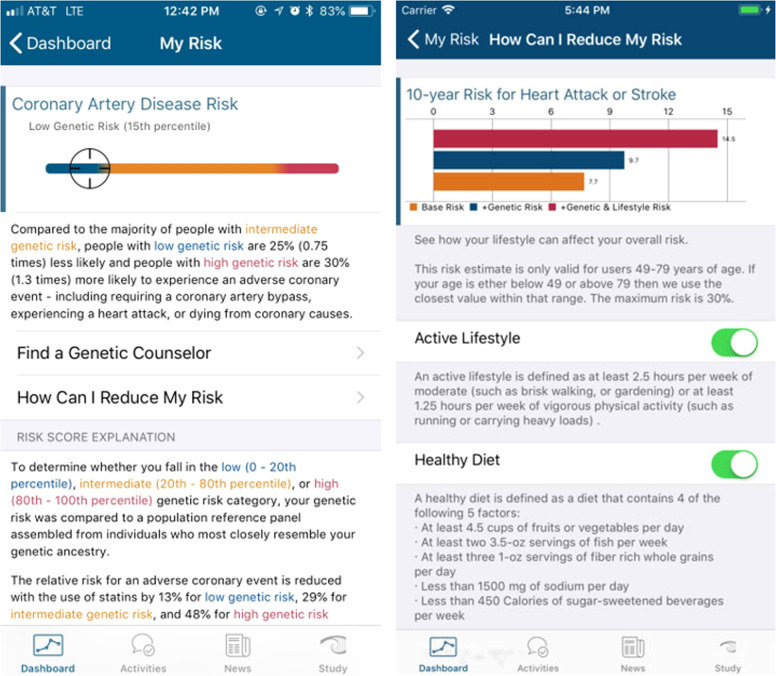
We developed a smartphone application, MyGeneRank, to conduct a prospective observational cohort study (NCT03277365) involving the automated generation, communication, and electronic capture of response to a polygenic risk score (PRS) for coronary artery disease (CAD). Adults with a smartphone and an existing 23andMe genetic profiling self-referred to the study. We evaluated self-reported actions taken in response to personal CAD PRS information, with special interest in the initiation of lipid-lowering therapy. 19% (721/3,800) of participants provided complete responses for baseline and follow-up use of lipid-lowering therapy. 20% (n = 19/95) of high CAD PRS vs 7.9% (n = 8/101) of low CAD PRS participants initiated lipid-lowering therapy at follow-up (p-value = 0.002). Both the initiation of statin and non-statin lipid-lowering therapy was associated with degree of CAD PRS: 15.2% (n = 14/92) vs 6.0% (n = 6/100) for statins (p-value = 0.018) and 6.8% (n = 8/118) vs 1.6% (n = 2/123) for non-statins (p-value = 0.022) in high vs low CAD PRS, respectively. High CAD PRS was also associated with earlier initiation of lipid lowering therapy (average age of 52 vs 65 years in high vs low CAD PRS respectively, p-value = 0.007). Overall, degree of CAD PRS was associated with use of any lipid-lowering therapy at follow-up: 42.4% (n = 56/132) vs 28.5% (n = 37/130) (p-value = 0.009). We find that digital communication of personal CAD PRS information is associated with increased and earlier lipid-lowering initiation in individuals of high CAD PRS. Loss to follow-up is the primary limitation of this study. Alternative communication routes, and long-term studies with EHR-based outcomes are needed to understand the generalizability and durability of this finding.
我们开发了一款智能手机应用程序MyGeneRank,以开展一项前瞻性观察性队列研究(NCT03277365),该研究涉及对冠状动脉疾病(CAD)的多基因风险评分(PRS)的反应进行自动生成、传达及电子捕获。拥有智能手机且已有23andMe基因谱分析结果的成年人可自行报名参加该研究。我们评估了针对个人CAD PRS信息所采取的自我报告行动,特别关注降脂治疗的启动情况。19%(721/3800)的参与者提供了关于降脂治疗基线和随访使用情况的完整回复。高CAD PRS参与者中有20%(n = 19/95)在随访时启动了降脂治疗,而低CAD PRS参与者中这一比例为7.9%(n = 8/101)(p值 = 0.002)。他汀类和非他汀类降脂治疗的启动均与CAD PRS程度相关:高CAD PRS组中他汀类药物治疗的启动率为15.2%(n = 14/92),低CAD PRS组为6.0%(n = 6/100)(p值 = 0.018);高CAD PRS组中非他汀类药物治疗的启动率为6.8%(n = 8/118),低CAD PRS组为1.6%(n = 2/123)(p值 = 0.022)。高CAD PRS还与更早开始降脂治疗相关(高CAD PRS组的平均年龄为52岁,低CAD PRS组为65岁,p值 = 0.007)。总体而言,CAD PRS程度与随访时使用任何降脂治疗相关:42.4%(n = 56/132)对比28.5%(n = 37/130)(p值 = 0.009)。我们发现,个人CAD PRS信息的数字传达与高CAD PRS个体中降脂治疗的增加及更早启动相关。失访是本研究的主要局限性。需要采用替代沟通途径以及基于电子健康记录(EHR)结果的长期研究,以了解这一发现的普遍性和持久性。