Arai Nobuyuki, Abe Hiromasa, Nishitani Haruhiko, Kanemaru Shimon, Yasunaga Masaru, Yamamoto Sayako, Seki Sousuke, Metani Hiromichi, Hiraoka Takashi, Hanayama Kozo
Department of Rehabilitation Medicine, Kawasaki Medical School, Okayama, Japan.
Prog Rehabil Med. 2022 Feb 23;7:20220008. doi: 10.2490/prm.20220008. eCollection 2022.
This study retrospectively investigated the prevalence and clinical features of trephine syndrome, which is a late complication of craniectom, in patients who underwent craniectomy decompression.
Trephine syndrome was defined as an increase of ≥2 points in the functional independent measure (FIM) score at 7 days after cranioplasty compared with that 3 days before cranioplasty. Patients who underwent craniectomy at Kawasaki Medical School Hospital between January 1, 2010, and March 15, 2020, were included in the study.
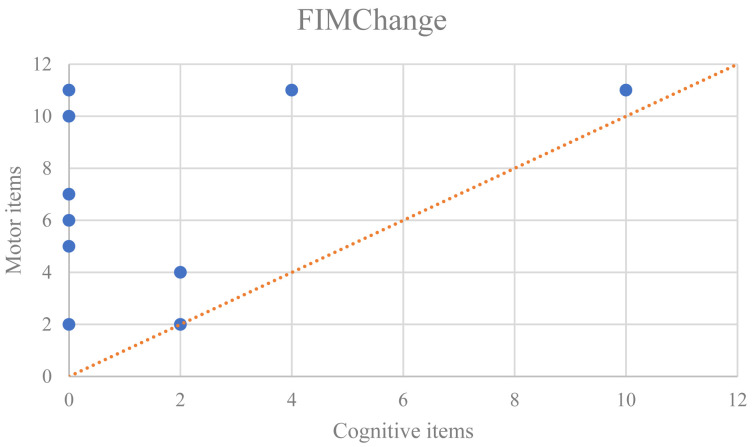
During the observation period, 102 patients underwent craniectomy decompression; 71 of them later underwent cranioplasty. In total, 12 and 59 patients were assigned to the trephine and non-trephine syndrome groups, respectively. The patients in the trephine syndrome group were significantly younger than those in the non-trephine syndrome group (P<0.05). The mean durations±standard deviations (in days) from craniectomy decompression to cranioplasty were 57.1±38.9 and 83.6±69.3 for the trephine and non-trephine syndrome groups, respectively (P<0.05). Improvements in the FIM motor scores were greater than the improvements in the cognitive scores for all but one case (P<0.05). The frequency with which patients experienced exacerbation (worsened consciousness and sudden anisocoria) after hospitalization was significantly higher in the trephine syndrome group than in the non-trephine syndrome group (P<0.05).
Performing cranioplasty as early as possible in young patients may lead to functional improvement. In the trephine syndrome group, the improvement in motor FIM score was greater than that of the cognitive score. Moreover, post-hospitalization exacerbation was more frequent in the trephine syndrome group.
本研究回顾性调查了颅骨切除术减压患者中作为颅骨切除术晚期并发症的环锯综合征的患病率及临床特征。
环锯综合征定义为颅骨修补术后7天的功能独立性测量(FIM)评分较颅骨修补术前3天增加≥2分。2010年1月1日至2020年3月15日期间在川崎医科大学医院接受颅骨切除术的患者纳入本研究。
观察期间,102例患者接受了颅骨切除术减压;其中71例随后接受了颅骨修补术。总共分别有12例和59例患者被归入环锯综合征组和非环锯综合征组。环锯综合征组患者明显比非环锯综合征组患者年轻(P<0.05)。环锯综合征组和非环锯综合征组从颅骨切除术减压到颅骨修补术的平均持续时间±标准差(天)分别为57.1±38.9和83.6±69.3(P<0.05)。除1例病例外,所有病例的FIM运动评分改善均大于认知评分改善(P<0.05)。环锯综合征组患者住院后病情加重(意识恶化和突然瞳孔不等大)的频率明显高于非环锯综合征组(P<0.05)。
年轻患者尽早进行颅骨修补术可能会带来功能改善。在环锯综合征组中,运动FIM评分的改善大于认知评分。此外,环锯综合征组住院后病情加重更为频繁。