From the Department of Medical Imaging, The Ottawa Hospital, University of Ottawa, Ottawa, Canada (N.S., R.M.H., C.W.); Departments of Radiology (M.S.D., D.B., N.E.C.) and Urology (M.S.D.), University of Michigan Medical Center, Ann Arbor, Mich; Department of Radiology, Brigham and Women's Hospital, Harvard Medical School, Boston, Mass (S.G.S., I.G., A.B.S.); Department of Radiology, NYU Langone Medical Center, New York, NY (B.B., A.M.D., N.H.); Department of Radiology, University of Nebraska Medical Center, Omaha, Neb (Z.B., R.T.D., E.E., E.G.); Department of Epidemiology, Ottawa Hospital Research Institute, Ottawa, Canada (T.R.); and Departments of Radiology and Urology, Advanced Imaging Research Center, University of Texas Southwestern Medical Center, 2201 Inwood Rd, 2nd Floor, Suite 202, Dallas, TX 75390-9085 (I.P.).
Radiology. 2022 Jun;303(3):590-599. doi: 10.1148/radiol.211680. Epub 2022 Mar 15.
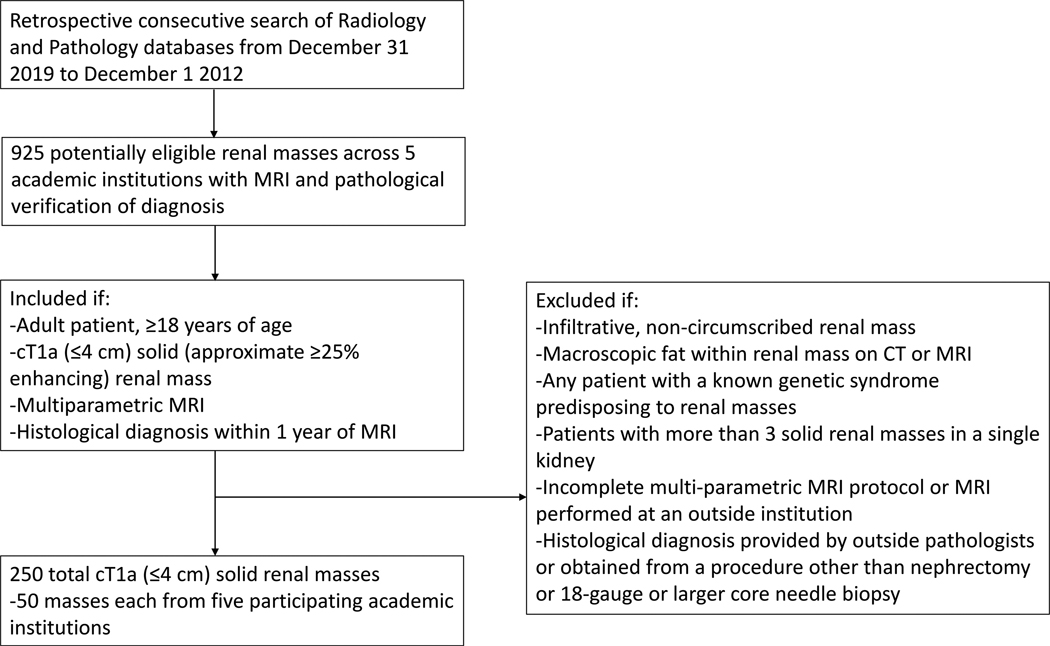
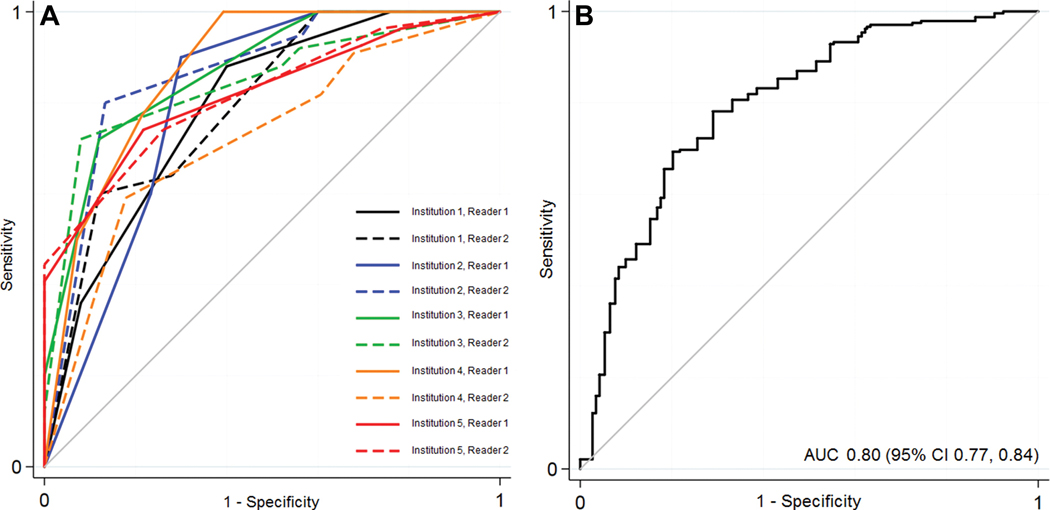
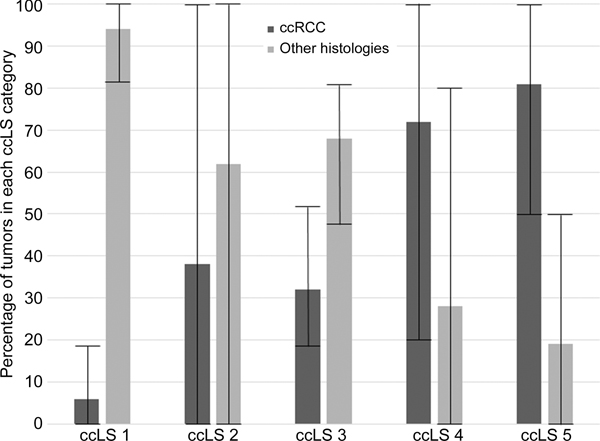
Background Solid small renal masses (SRMs) (≤4 cm) represent benign and malignant tumors. Among SRMs, clear cell renal cell carcinoma (ccRCC) is frequently aggressive. When compared with invasive percutaneous biopsies, the objective of the proposed clear cell likelihood score (ccLS) is to classify ccRCC noninvasively by using multiparametric MRI, but it lacks external validation. Purpose To evaluate the performance of and interobserver agreement for ccLS to diagnose ccRCC among solid SRMs. Materials and Methods This retrospective multicenter cross-sectional study included patients with consecutive solid (≥25% approximate volume enhancement) SRMs undergoing multiparametric MRI between December 2012 and December 2019 at five academic medical centers with histologic confirmation of diagnosis. Masses with macroscopic fat were excluded. After a 1.5-hour training session, two abdominal radiologists per center independently rendered a ccLS for 50 masses. The diagnostic performance for ccRCC was calculated using random-effects logistic regression modeling. The distribution of ccRCC by ccLS was tabulated. Interobserver agreement for ccLS was evaluated with the Fleiss κ statistic. Results A total of 241 patients (mean age, 60 years ± 13 [SD]; 174 men) with 250 solid SRMs were evaluated. The mean size was 25 mm ± 8 (range, 10-39 mm). Of the 250 SRMs, 119 (48%) were ccRCC. The sensitivity, specificity, and positive predictive value for the diagnosis of ccRCC when ccLS was 4 or higher were 75% (95% CI: 68, 81), 78% (72, 84), and 76% (69, 81), respectively. The negative predictive value of a ccLS of 2 or lower was 88% (95% CI: 81, 93). The percentages of ccRCC according to the ccLS were 6% (range, 0%-18%), 38% (range, 0%-100%), 32% (range, 60%-83%), 72% (range, 40%-88%), and 81% (range, 73%-100%) for ccLSs of 1-5, respectively. The mean interobserver agreement was moderate (κ = 0.58; 95% CI: 0.42, 0.75). Conclusion The clear cell likelihood score applied to multiparametric MRI had moderate interobserver agreement and differentiated clear cell renal cell carcinoma from other solid renal masses, with a negative predictive value of 88%. © RSNA, 2022 See also the editorial by Mileto and Potretzke in this issue.
背景 实体小肾脏肿块(SRMs)(≤4 cm)代表良性和恶性肿瘤。在 SRMs 中,透明细胞肾细胞癌(ccRCC)通常具有侵袭性。与侵入性经皮活检相比,提出的透明细胞可能性评分(ccLS)的目的是通过使用多参数 MRI 对 ccRCC 进行非侵入性分类,但缺乏外部验证。目的 评估 ccLS 用于诊断实体 SRMs 中 ccRCC 的性能和观察者间一致性。材料与方法 本回顾性多中心横断面研究纳入了 2012 年 12 月至 2019 年 12 月在五家学术医疗中心接受多参数 MRI 检查的连续实体(≥25%近似体积增强)SRMs 患者,且经组织学证实诊断。排除有肉眼脂肪的肿块。在 1.5 小时的培训课程后,每个中心的两名腹部放射科医生分别对 50 个肿块进行 ccLS 评分。使用随机效应逻辑回归模型计算 ccRCC 的诊断性能。通过 ccLS 对 ccRCC 进行制表。使用 Fleiss κ 统计量评估 ccLS 的观察者间一致性。结果 共评估了 241 名患者(平均年龄 60 岁±13[SD];174 名男性)的 250 个实体 SRMs。平均大小为 25 mm±8(范围,10-39 mm)。在 250 个 SRMs 中,119 个(48%)为 ccRCC。当 ccLS 为 4 或更高时,ccRCC 诊断的灵敏度、特异性和阳性预测值分别为 75%(95%CI:68,81)、78%(72,84)和 76%(69,81)。ccLS 为 2 或更低时的阴性预测值为 88%(95%CI:81,93)。根据 ccLS,ccRCC 的百分比分别为 6%(范围,0%-18%)、38%(范围,0%-100%)、32%(范围,60%-83%)、72%(范围,40%-88%)和 81%(范围,73%-100%)ccLS 为 1-5。观察者间平均一致性为中度(κ=0.58;95%CI:0.42,0.75)。结论 应用于多参数 MRI 的透明细胞可能性评分具有中度的观察者间一致性,并能区分透明细胞肾细胞癌和其他实体肾肿块,阴性预测值为 88%。©RSNA,2022 另请参见本期 Mileto 和 Potretzke 的社论。