Department of Medicine, Emory University School of Medicine, Atlanta, GA, USA.
Department of Biostatistics and Bioinformatics Shared Resource, Winship Cancer Institute, Emory University, Atlanta, GA, USA.
Oncologist. 2022 Feb 3;27(1):48-56. doi: 10.1093/oncolo/oyab001.
The eighth edition American Joint Committee on Cancer (AJCC) Staging incorporates significant changes to the seventh edition in the staging of oropharyngeal squamous cell carcinomas (OPSCC). An important change was the inclusion of OPSCC associated with the human papilloma virus (HPV). Our goal is to compare the performance of both staging systems for patients with HPV-selected and unselected clinical characteristics for OPSCC.
Using the Surveillance, Epidemiology, and End Results (SEER) database, 2004-2016, we identified patients with likely HPV-associated OPSCC based on surrogate markers (white males aged <65 years old with squamous cell carcinomas of the tonsil and base of tongue), excluding those who underwent surgery. We re-classified these patients using seventh and eighth edition staging for HPV-selected OPSCC and compared the prediction performance of both staging editions for overall survival (OS) and disease-specific survival (DSS). We performed the same analysis for clinically unselected patients with OPSCC.
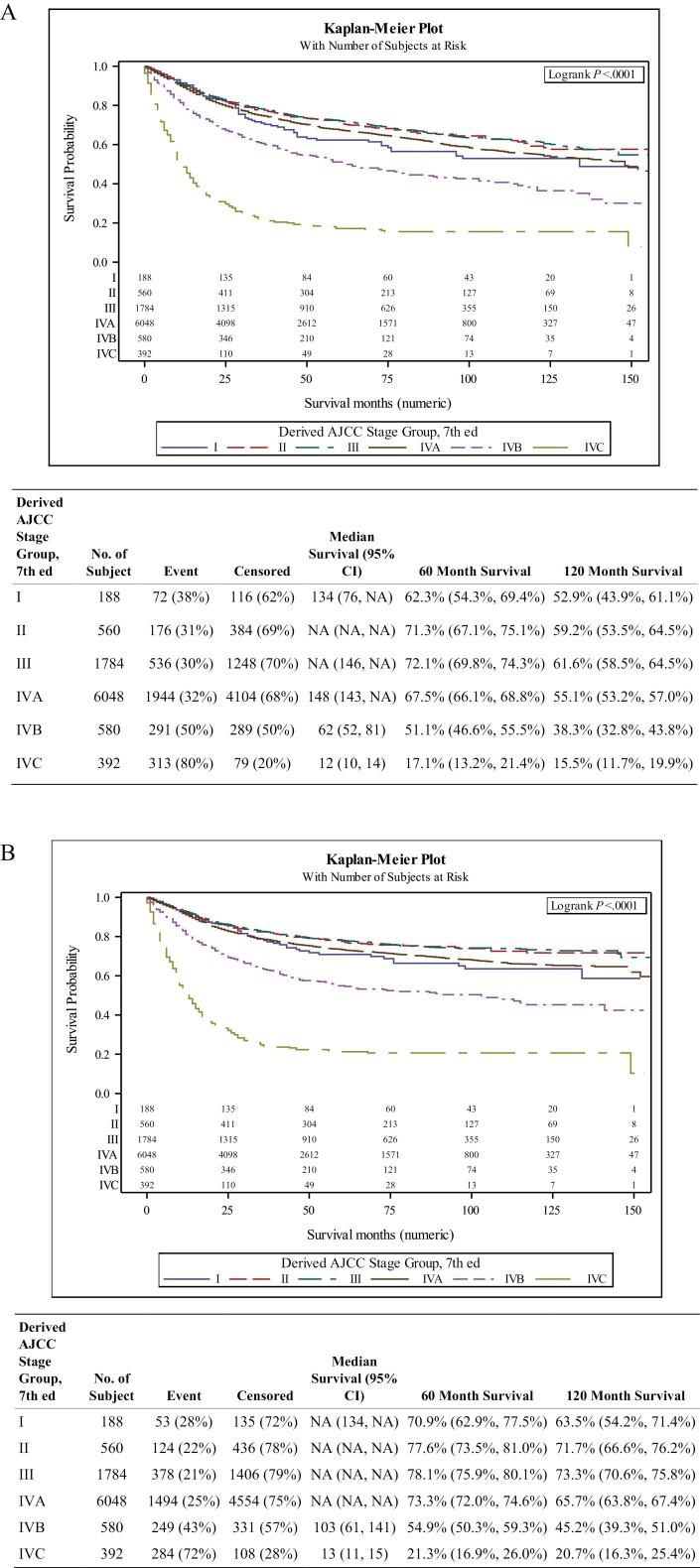
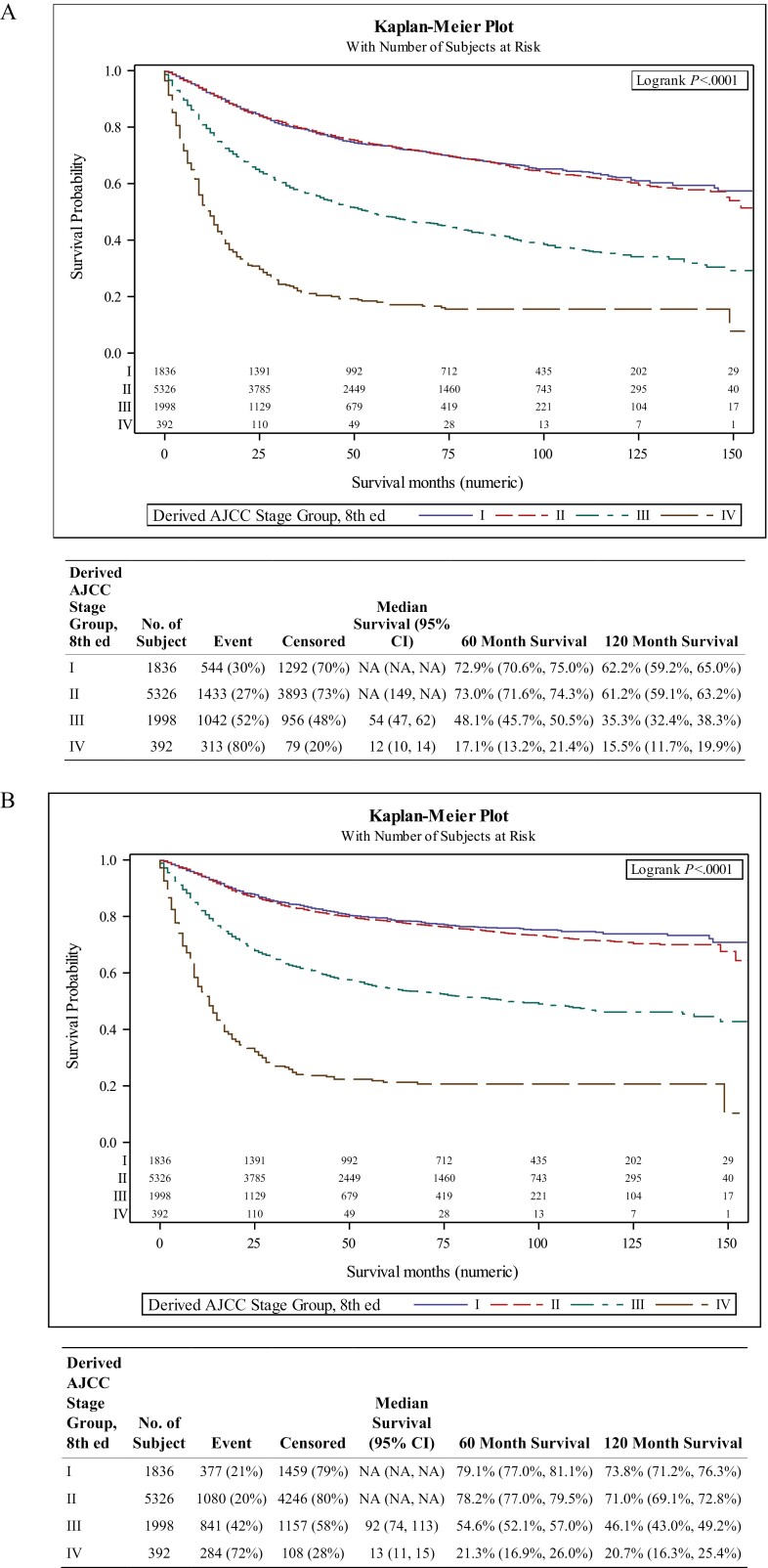
Our analysis included 9554 patients with a median follow-up of 67 months. Comparing the eighth versus seventh edition for our HPV-selected cohort, clinical staging changed for 92.3% of patients and 10-year OS was 62.2%, 61.2%, 35.3%, and 15.5% for Stage I, II, III, and IV, versus 52.9%, 59.2%, 61.6%, 55.1%, 38.3%, and 15.5% for stage I, II, III, IVA, IVB, and IVC, respectively. A similar pattern was observed for 10-year DSS. The concordance statistics for our HPV-selected cohort were improved for both AJCC 7 (0.6260) and AJCC 8 (0.6846) compared with the unselected cohort, 0.5860 and 0.6457 for AJCC 7 and 8, respectively.
The overall performance of discrimination improved from AJCC 7 to AJCC 8 for both clinically selected and unselected patients, but more notably for our HPV-selected cohort. Despite the lack of statistically significant differentiation between Stages I and II in AJCC 8 in either groups, markedly improved discrimination was observed between Stages I/II, III, and IV in the HPV-selected cohort.
第八版美国癌症联合委员会(AJCC)分期在口咽鳞状细胞癌(OPSCC)分期方面对第七版进行了重大修改。一个重要的变化是包括了与人类乳头瘤病毒(HPV)相关的 OPSCC。我们的目标是比较两种分期系统在 HPV 选择和非选择临床特征的 OPSCC 患者中的表现。
利用监测、流行病学和最终结果(SEER)数据库,2004 年至 2016 年,我们根据替代标志物(<65 岁的白人男性,扁桃体和舌根的鳞状细胞癌),排除接受手术的患者,确定了可能与 HPV 相关的 OPSCC 患者。我们使用第七和第八版分期对这些患者进行了再分类,比较了两种分期系统对总生存(OS)和疾病特异性生存(DSS)的预测性能。我们对 OPSCC 的临床未选择患者进行了相同的分析。
我们的分析包括 9554 名患者,中位随访时间为 67 个月。比较第八版与第七版我们的 HPV 选择队列,92.3%的患者临床分期发生改变,10 年 OS 为 I 期 62.2%、II 期 61.2%、III 期 35.3%、IV 期 15.5%,而 I 期、II 期、III 期、IVA 期、IVB 期和 IVC 期分别为 52.9%、59.2%、61.6%、55.1%、38.3%和 15.5%。DSS 也观察到类似的模式。与未选择的队列相比,我们 HPV 选择队列的 AJCC 7(0.6260)和 AJCC 8(0.6846)的一致性统计数据有所提高,分别为 0.5860 和 0.6457。
对于临床选择和未选择的患者,从 AJCC 7 到 AJCC 8 的整体判别性能均有所提高,但对于我们的 HPV 选择队列更为显著。尽管在两个队列中 AJCC 8 的 I 期和 II 期之间没有统计学上的显著差异,但在 HPV 选择队列中,I/II 期、III 期和 IV 期之间的判别能力显著提高。