Neonatal Intensive Care Centre, King's College Hospital NHS Foundation Trust, London, UK.
Women and Children's Health, School of Life Course Sciences, Faculty of Life Sciences and Medicine, King's College London, London, UK.
Pediatr Res. 2022 Dec;92(6):1657-1662. doi: 10.1038/s41390-022-02001-2. Epub 2022 Mar 19.
We aimed to explore the postnatal evolution of ventilation/perfusion ratio (V/Q) and right-to-left shunt in infants with congenital diaphragmatic hernia (CDH) and whether these indices predicted survival to discharge.
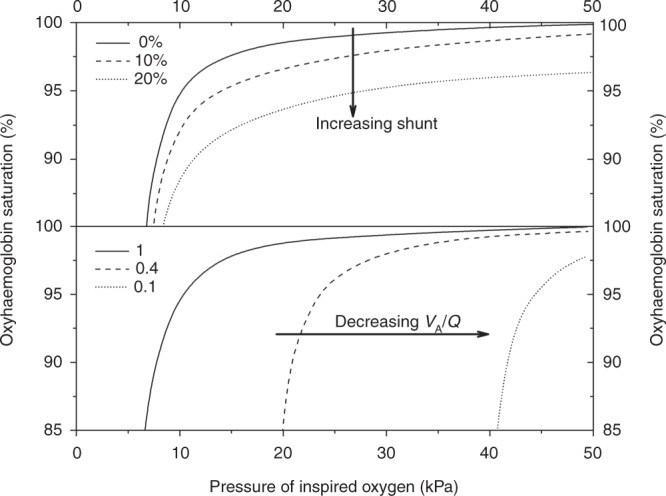
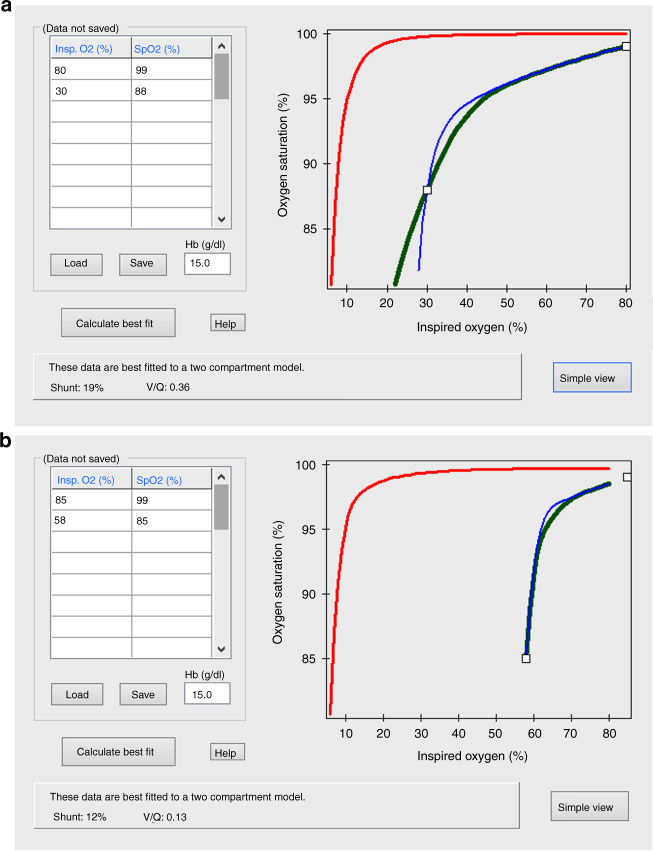
Retrospective cohort study at King's College Hospital, London, UK of infants admitted with CDH in 10 years (2011-2021). The non-invasive method of the oxyhaemoglobin dissociation curve was used to determine the V/Q and shunt in the first 24 h of life, pre-operation, pre-extubation and in the deceased infants, before death.
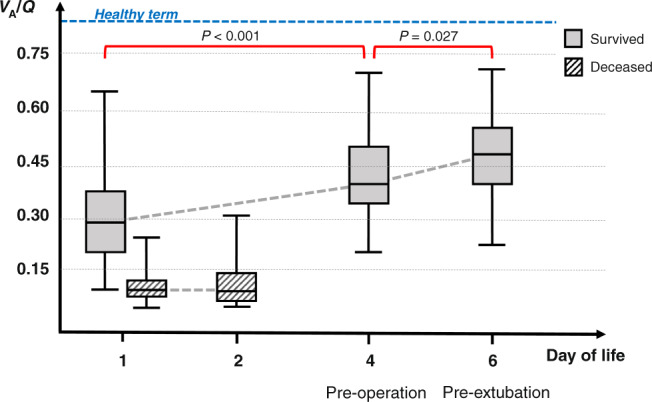
Eighty-two infants with CDH (71 left-sided) were included with a median (IQR) gestation of 38.1(34.8-39.0) weeks. Fifty-three (65%) survived to discharge from neonatal care. The median (IQR) V/Q in the first 24 h was lower in the deceased infants [0.09(0.07-0.12)] compared to the ones who survived [0.28(0.19-0.38), p < 0.001]. In the infants who survived, the V/Q was lower in the first 24 h [0.28 (0.19-0.38)] compared to pre-operation [0.41 (0.3-0.49), p < 0.001] and lower pre-operation compared to pre-extubation [0.48 (0.39-0.55), p = 0.027]. The shunt was not different in infants who survived compared to the infants who did not.
Ventilation-to-perfusion ratio was lower in infants who died in the neonatal period compared to the ones that survived and improved in surviving infants over the immediate postnatal period.
The non-invasive method of the oxyhaemoglobin dissociation curve was used to determine the ventilation/perfusion ratio V/Q in infants with congenital diaphragmatic hernia (CDH) in the first 24 h of life, pre-operation, pre-extubation and in the deceased infants, before death. The V/Q in the first 24 h of life was lower in the infants who did not survive to discharge from neonatal care compared to the ones who survived. In the infants who survived, the V/Q improved over the immediate postnatal period. The non-invasive calculation of V/Q can provide valuable information relating to survival to discharge.
我们旨在探讨先天性膈疝(CDH)患儿出生后通气/灌注比(V/Q)和右向左分流的演变情况,以及这些指标是否可预测患儿的存活至出院。
这是英国伦敦国王学院医院的一项回顾性队列研究,纳入了 10 年间(2011 年至 2021 年)患有 CDH 的婴儿。使用氧合血红蛋白解离曲线的非侵入性方法,在出生后 24 小时内、术前、拔管前和死亡前,确定 V/Q 和分流情况。
共纳入 82 例 CDH 婴儿(71 例左侧),中位(IQR)胎龄为 38.1(34.8-39.0)周。53 例(65%)存活至新生儿重症监护病房出院。与存活的患儿相比,死亡患儿出生后 24 小时内的 V/Q 中位数[0.09(0.07-0.12)]较低(p<0.001)。在存活的患儿中,出生后 24 小时内的 V/Q 中位数[0.28(0.19-0.38)]较术前[0.41(0.3-0.49)]较低(p<0.001),术前 V/Q 较拔管前[0.48(0.39-0.55)]较低(p=0.027)。与存活的患儿相比,死亡患儿的分流情况无差异。
与存活的患儿相比,在新生儿期死亡的患儿的通气/灌注比值较低,且在存活的患儿中,该比值在出生后的即刻后期有所改善。
本研究使用氧合血红蛋白解离曲线的非侵入性方法,在先天性膈疝(CDH)患儿出生后 24 小时内、术前、拔管前和死亡前,确定 V/Q。与存活至新生儿重症监护病房出院的患儿相比,出生后 24 小时内未存活的患儿的 V/Q 较低。在存活的患儿中,V/Q 在出生后的即刻后期有所改善。V/Q 的非侵入性计算可以提供与存活至出院相关的有价值的信息。