Hwang Jeong Ah, Song Younghoon, Shin Jaeun, Cho Eunjung, Ahn Shin Young, Ko Gang Jee, Kwon Young Joo, Kim Ji Eun
Department of Internal Medicine, Korea University Guro Hospital, Seoul, South Korea.
Department of Internal Medicine, Korea University College of Medicine, Seoul, South Korea.
Front Med (Lausanne). 2022 Mar 2;9:810901. doi: 10.3389/fmed.2022.810901. eCollection 2022.
Serum creatinine and cystatin C are not only good indicators of renal function but have also been confirmed to be related to disease prognosis and mortality in various diseases via creatinine/cystatin C ratio (CCR). However, although they are biomarkers of renal function, there is no study regarding renal impairment as a confounding variable in the relationship between CCR and all-cause mortality.
Patients who had simultaneous measurements of serum creatinine and cystatin C between 2003 and 2020 were enrolled. The patients with chronic kidney disease (CKD) were defined as having an estimated glomerular filtration rate (eGFR) CKD-EPI Cr-Cystatin C < 60 ml/min/1.73 m. CCR was calculated by dividing the serum creatinine level by the cystatin C level measured on the same day. The main outcome assessed was all-cause mortality according to CCR in CKD or non-CKD groups.
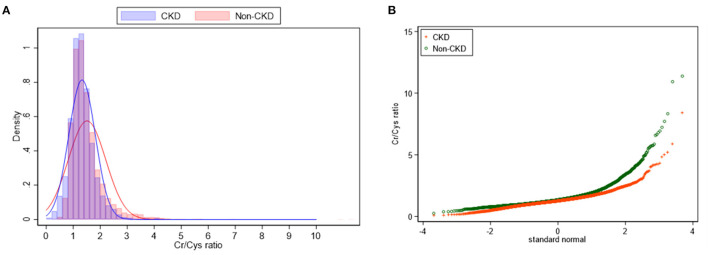
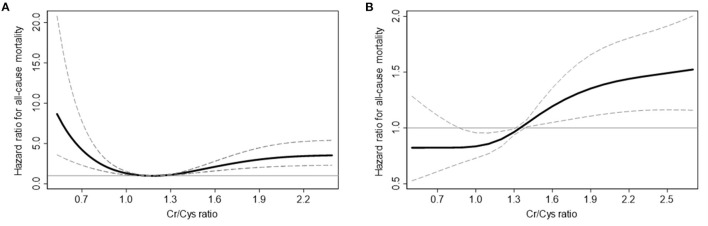
Among the 8,680 patients in whom creatinine and cystatin C levels were measured simultaneously, 4,301 were included in the CKD group, and 4,379 were included in the non-CKD group, respectively. CCR was 1.4 ± 0.6 in total participants. The non-CKD group showed higher mean CCR, (1.5 ± 0.7 vs. 1.3 ± 0.5) as well as a wider distribution of CCR ( < 0.001) when compared to the CKD group. In non-CKD group, 1, 4 and 5 quintiles of CCR significantly increased the all-cause mortality risk compared to 2 quintile of CCR, suggesting U-shaped mortality risk according to CCR in non-CKD. On the other hand, in CKD group, the risk of all-cause mortality linearly increased and 5 quintile of CCR showed 1.82 times risk of mortality compared to 2 quintile of CCR. In the subgroup analysis of mortality by age and sex, the mortality difference according to CCR were diminished in old age and female sex subgroups.
We discovered a U-shaped relationship between mortality and CCR levels in normal renal function, and an increased risk of mortality in CKD with elevated CCR.
血清肌酐和胱抑素C不仅是肾功能的良好指标,而且通过肌酐/胱抑素C比值(CCR)已被证实与各种疾病的疾病预后和死亡率相关。然而,尽管它们是肾功能的生物标志物,但尚无关于肾功能损害作为CCR与全因死亡率之间关系的混杂变量的研究。
纳入2003年至2020年期间同时测量血清肌酐和胱抑素C的患者。慢性肾脏病(CKD)患者定义为估算肾小球滤过率(eGFR)CKD-EPI Cr-胱抑素C<60 ml/min/1.73 m²。CCR通过将血清肌酐水平除以同一天测量的胱抑素C水平来计算。评估的主要结局是CKD组或非CKD组中根据CCR的全因死亡率。
在同时测量肌酐和胱抑素C水平的8680例患者中,CKD组纳入4301例,非CKD组纳入4379例。所有参与者的CCR为1.4±0.6。与CKD组相比,非CKD组的平均CCR更高(1.5±0.7对1.3±0.5),CCR的分布也更广(P<0.001)。在非CKD组中,与CCR的第2五分位数相比,CCR的第1、第4和第5五分位数显著增加了全因死亡风险,表明非CKD组中根据CCR存在U形死亡风险。另一方面,在CKD组中,全因死亡风险呈线性增加,与CCR的第2五分位数相比,CCR的第5五分位数显示死亡风险为1.82倍。在按年龄和性别进行的死亡率亚组分析中,老年和女性亚组中根据CCR的死亡率差异减小。
我们发现正常肾功能中死亡率与CCR水平之间存在U形关系,且CCR升高的CKD患者死亡风险增加。