Iwasaki Makoto, Kanda Junya, Tanaka Hidenori, Shindo Takero, Sato Takahiko, Doki Noriko, Fukuda Takahiro, Ozawa Yukiyasu, Eto Tetsuya, Uchida Naoyuki, Katayama Yuta, Kataoka Keisuke, Ara Takahide, Ota Shuichi, Onizuka Makoto, Kanda Yoshinobu, Ichinohe Tatsuo, Atsuta Yoshiko, Morishima Satoko
Department of Hematology and Oncology, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
HLA Foundation Laboratory, Kyoto, Japan.
Front Immunol. 2022 Mar 3;13:811733. doi: 10.3389/fimmu.2022.811733. eCollection 2022.
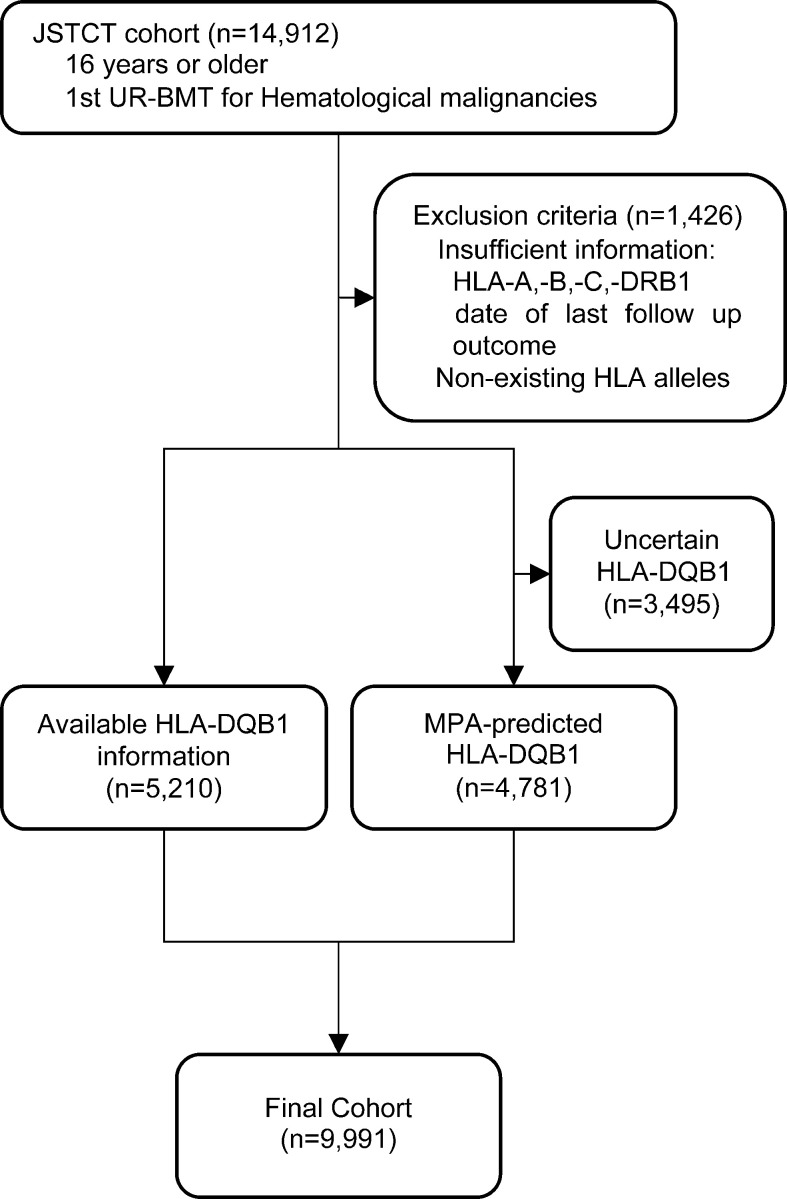
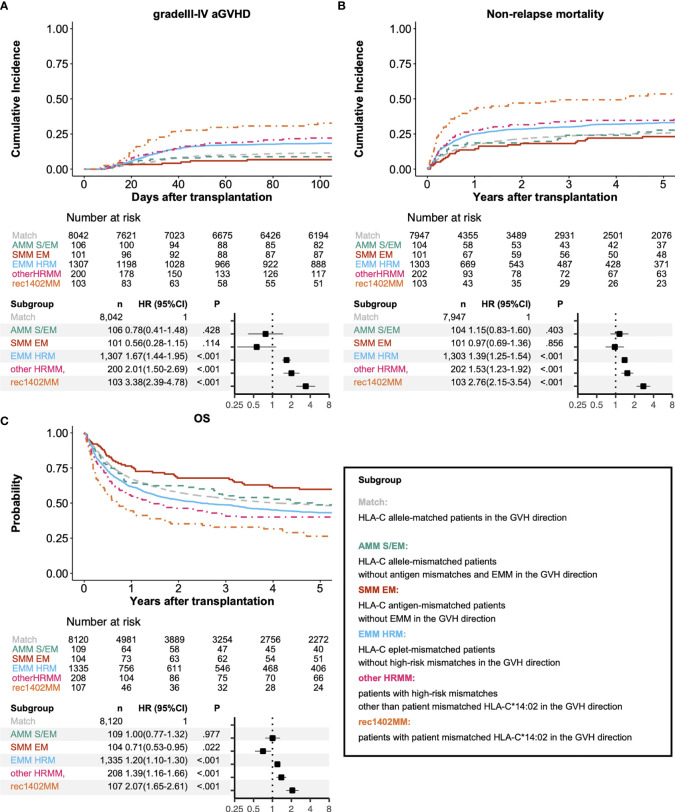
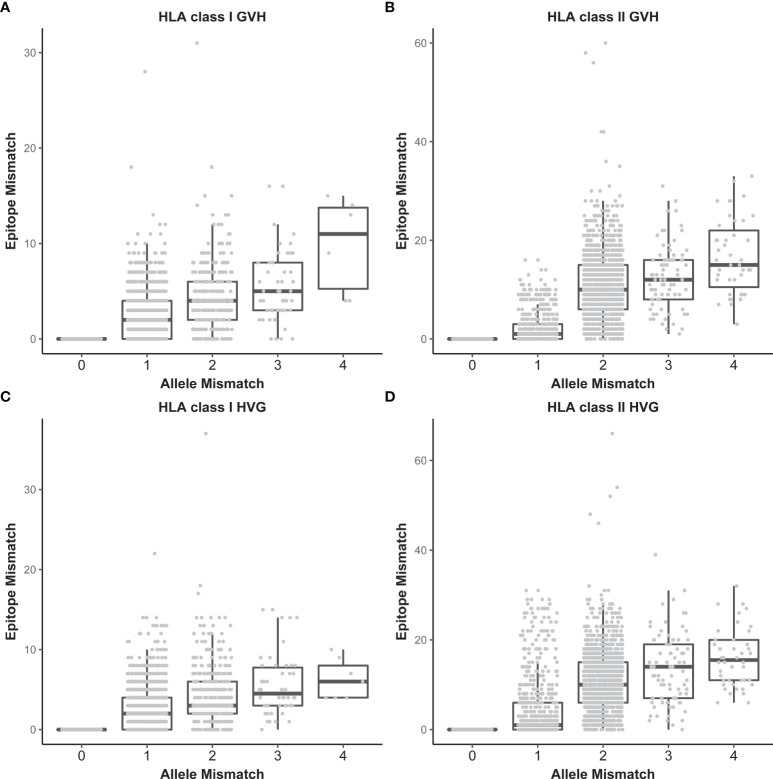
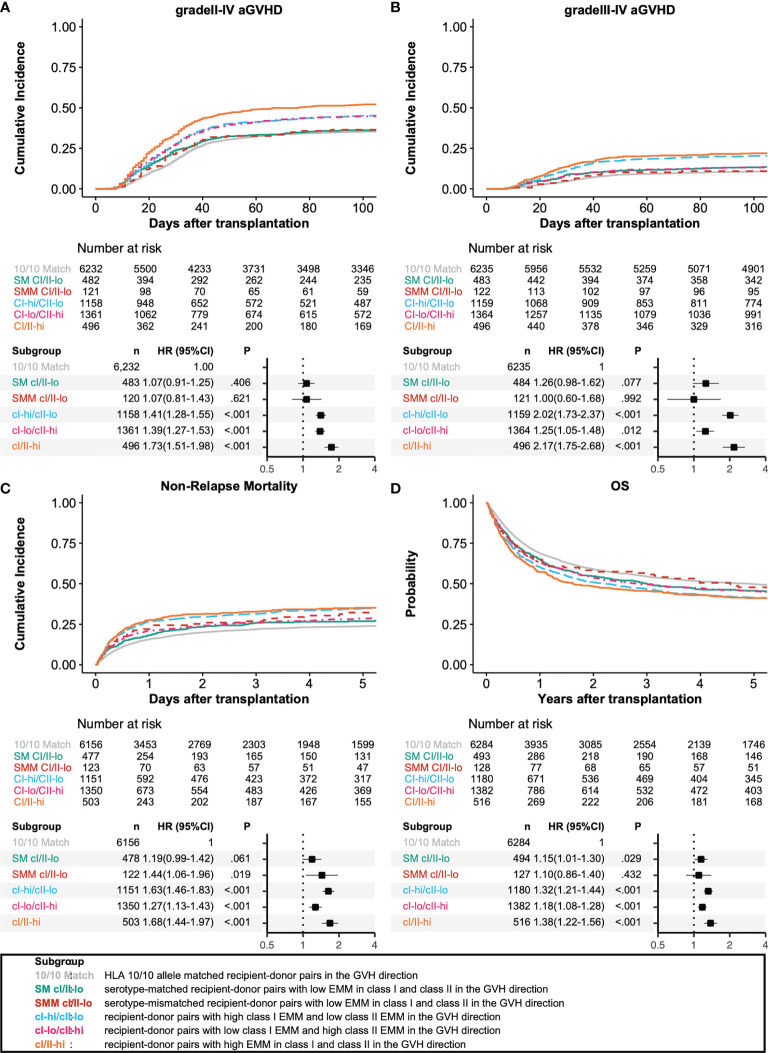
The significance of antibody-identified epitopes stimulating humoral alloimmunity is not well understood in the identification of non-permissive human leukocyte antigen (HLA) mismatching patterns in hematopoietic stem cell transplantation (HSCT). This was a retrospective study in a cohort of 9,991 patients who underwent their first HSCT for hematologic malignancies from unrelated bone marrow donors in the Transplant Registry Unified Management Program (TRUMP). HLA eplet mismatches (EMM) were quantified using HLAMatchmaker (HLAMM). The median age of patients was 48 years (range, 16 to 77). The number of EMM in recipient-donor pairs in our study population ranged from 0 to 37 in HLA class I (median, 0) and 0 to 60 in HLA class II (median, 1). In addition to the known high-risk mismatch patterns in the Japanese cohort, HLA-C EMM in the GVH direction was associated with a significantly higher risk for grade III-IV aGVHD, leading to a higher risk of non-relapse mortality and lower overall survival (compared with HLA-C matched patients, HR 1.67, 95% CI 1.44-1.95; HR 1.39, 95% CI 1.25-1.54; HR 1.20, 95% CI 1.10-1.30, respectively). HLAMM-based epitope matching might be useful for identifying patients who are at high risk for serious complications after HSCT from HLA mismatched unrelated donors.
在造血干细胞移植(HSCT)中,抗体识别的表位刺激体液同种免疫的意义在非允许性人类白细胞抗原(HLA)错配模式的识别中尚未得到充分理解。这是一项对9991例患者的回顾性研究,这些患者在移植登记统一管理计划(TRUMP)中接受了来自无关骨髓供体的首次HSCT,用于治疗血液系统恶性肿瘤。使用HLAMatchmaker(HLAMM)对HLA表位错配(EMM)进行量化。患者的中位年龄为48岁(范围16至77岁)。在我们的研究人群中,受体-供体对中HLA I类的EMM数量范围为0至37(中位数为0),HLA II类为0至60(中位数为1)。除了日本队列中已知的高风险错配模式外,GVH方向的HLA-C EMM与III-IV级急性移植物抗宿主病(aGVHD)的风险显著更高相关,导致非复发死亡率更高和总生存率更低(与HLA-C匹配的患者相比,HR分别为1.67,95%CI 1.44-1.95;HR 1.39,95%CI 1.25-1.54;HR 1.20,95%CI 1.10-1.30)。基于HLAMM的表位匹配可能有助于识别在接受HLA错配无关供体的HSCT后发生严重并发症风险较高的患者。