Mayerhofer Ernst, Kanz Dirk, Guschlbauer Brigitte, Anderson Christopher D, Asmussen Alexander, Grundmann Sebastian, Strecker Christoph, Harloff Andreas
Department of Neurology and Neurophysiology, Faculty of Medicine, Medical Center-University of Freiburg, University of Freiburg, Freiburg, Germany.
Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States.
Front Neurol. 2022 Mar 4;13:836609. doi: 10.3389/fneur.2022.836609. eCollection 2022.
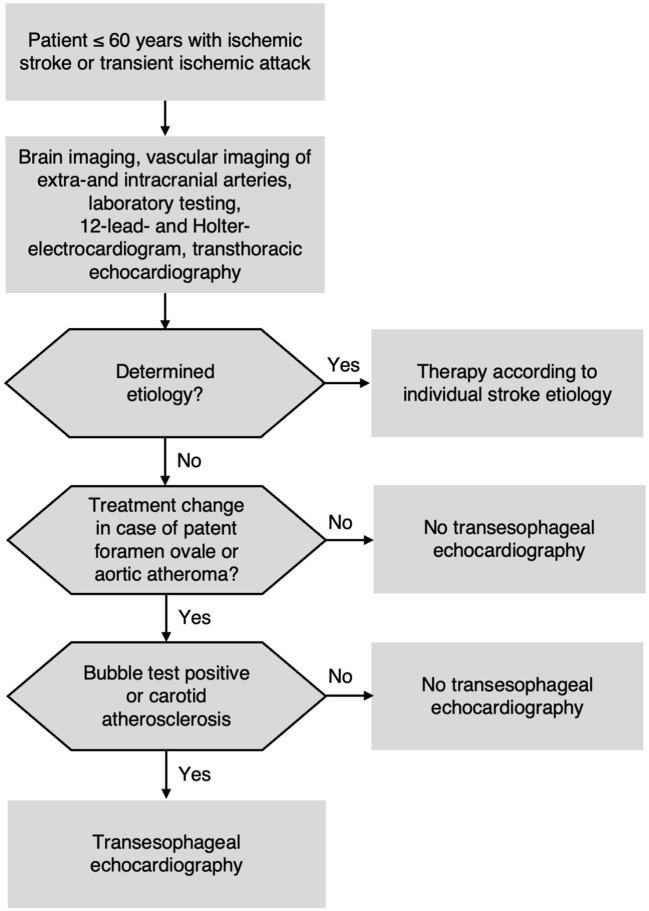
Indication of transesophageal echocardiography (TEE) in patients ≤60 years with brain ischemia is uncertain.
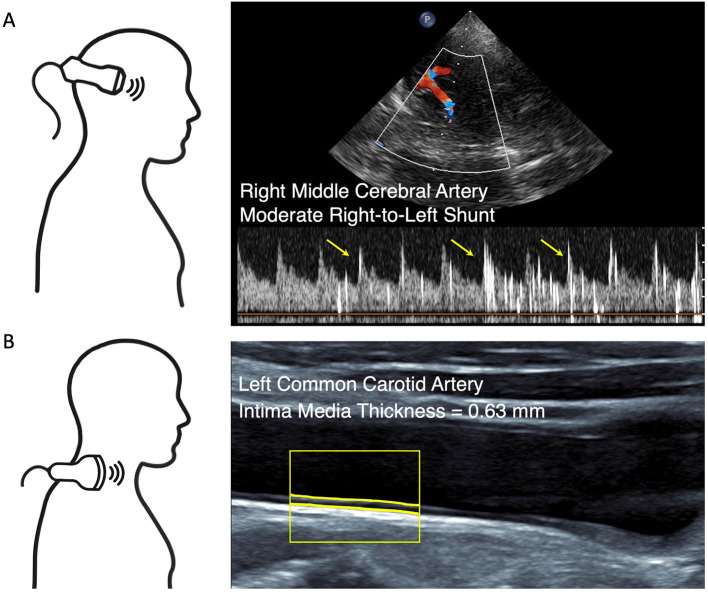
This prospective double-blinded study included patients with cryptogenic acute ischemic stroke or transient ischemic attack (TIA) ≥18 and ≤60 years. After routine diagnostics, all patients underwent patent foramen ovale (PFO) screening by transcranial Doppler (TCD) bubble test, carotid ultrasound for atherosclerosis screening (intima-media-thickness >0.90 mm or plaques), and TEE. We calculated sensitivity, specificity, positive predictive values (PPV), and negative predictive values (NPV) of the combined non-invasive ultrasound to predict therapy-relevant TEE findings.
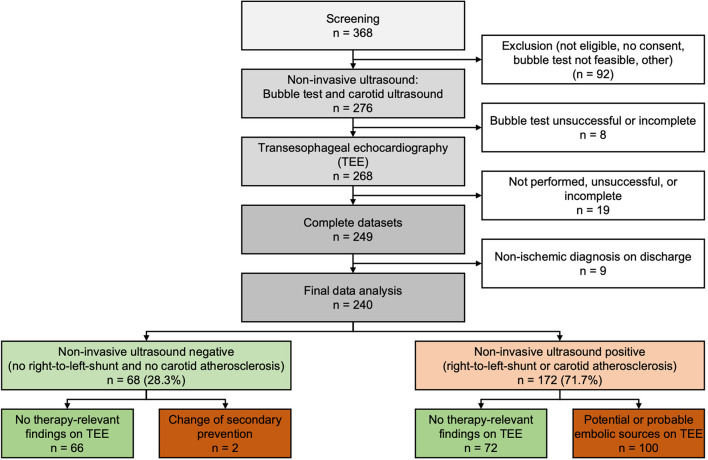
We included 240 consecutive patients (median 51 years, 39% women) of which 68 (28.3%) had both a negative bubble test and no carotid atherosclerosis. Of these, 66 (97.1%) had unremarkable TEE findings; in one patient a small PFO was found and closed subsequently, in another patient a 4.9 mm thick aortic atheroma was found, and double platelet inhibition initiated. Of the other 172 (71.7%) patients, 93 (54%) had PFO and 9 (5.2%) complex aortic plaques. No other therapy-relevant findings were present in both groups. Non-invasive ultrasound had a sensitivity of 98.0%, specificity of 47.8%, NPV of 97.1%, and PPV of 58.1% for therapy-relevant TEE findings.
Bubble test and carotid ultrasound could be used for the individual decision for/against TEE in patients with cryptogenic stroke ≤60 years. If they are unremarkable, TEE can be omitted with high safety regarding secondary prevention. If bubble test is positive and/or carotid ultrasound shows atherosclerosis, TEE should be carried out if PFO or aortic atheroma are potentially relevant for further patient management.
经食管超声心动图(TEE)在60岁及以下脑缺血患者中的应用指征尚不确定。
这项前瞻性双盲研究纳入了年龄在18岁至60岁之间的隐源性急性缺血性卒中或短暂性脑缺血发作(TIA)患者。在进行常规诊断后,所有患者均接受经颅多普勒(TCD)气泡试验以筛查卵圆孔未闭(PFO)、颈动脉超声以筛查动脉粥样硬化(内膜中层厚度>0.90mm或有斑块)以及TEE检查。我们计算了联合非侵入性超声预测与治疗相关的TEE检查结果的敏感性、特异性、阳性预测值(PPV)和阴性预测值(NPV)。
我们纳入了240例连续患者(中位年龄51岁,39%为女性),其中68例(28.3%)气泡试验阴性且无颈动脉粥样硬化。在这些患者中,66例(97.1%)TEE检查结果无异常;1例患者发现小的PFO并随后进行了封堵,另1例患者发现4.9mm厚的主动脉粥样瘤并启动了双重抗血小板抑制治疗。在其他172例(71.7%)患者中,93例(54%)有PFO,9例(5.2%)有复杂的主动脉斑块。两组均未发现其他与治疗相关的结果。对于与治疗相关的TEE检查结果,非侵入性超声的敏感性为98.0%,特异性为47.8%,NPV为97.1%,PPV为58.1%。
气泡试验和颈动脉超声可用于60岁及以下隐源性卒中患者是否进行TEE检查的个体化决策。如果检查结果无异常,在二级预防方面可高度安全地省略TEE检查。如果气泡试验阳性和/或颈动脉超声显示有动脉粥样硬化,若PFO或主动脉粥样瘤可能与患者的进一步管理相关,则应进行TEE检查。