Abraham Lucy, Halsby Kate, Stein Norman, Wrona Bozydar, Emir Birol, Stevenson Hannah
Pfizer Ltd., Surrey, UK.
NorthWest EHealth, Manchester, UK.
Rheumatol Ther. 2022 Jun;9(3):851-874. doi: 10.1007/s40744-022-00431-2. Epub 2022 Mar 21.
Using data from patients residing in Salford, UK, we aimed to compare healthcare resource utilisation (HCRU) and direct healthcare costs between patients with moderate to severe (M-S) or severe osteoarthritis (OA) pain and those without OA.
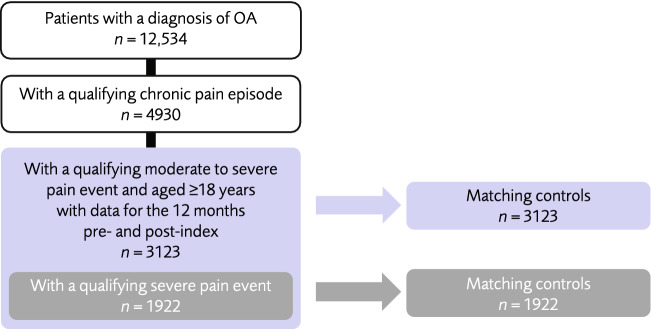
Patients with a M-S OA pain event within a period of chronic pain were indexed from the Salford Integrated Record (SIR) between 2010 and 2017. Patients with a severe pain event formed an OA subcohort. Patients in each OA pain cohort were independently matched to patients without OA, forming two control cohorts. HCRU, prescribed analgesic drugs, and total direct costs per UK standardised tariffs were calculated for the year post-index. Multivariable models were used to identify drivers of healthcare cost.
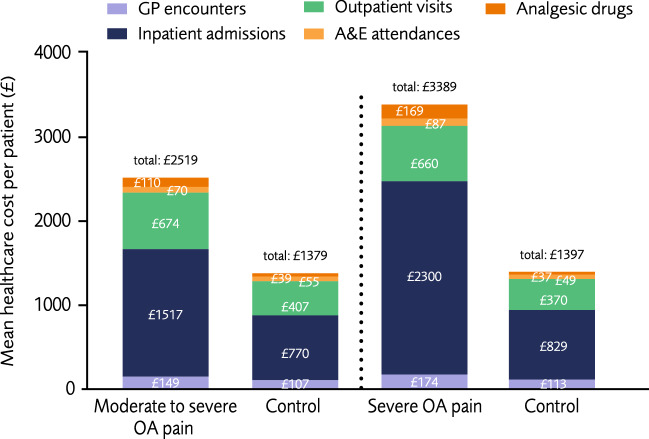
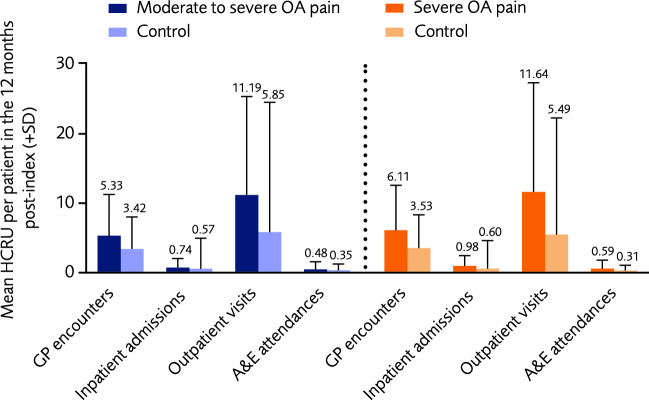
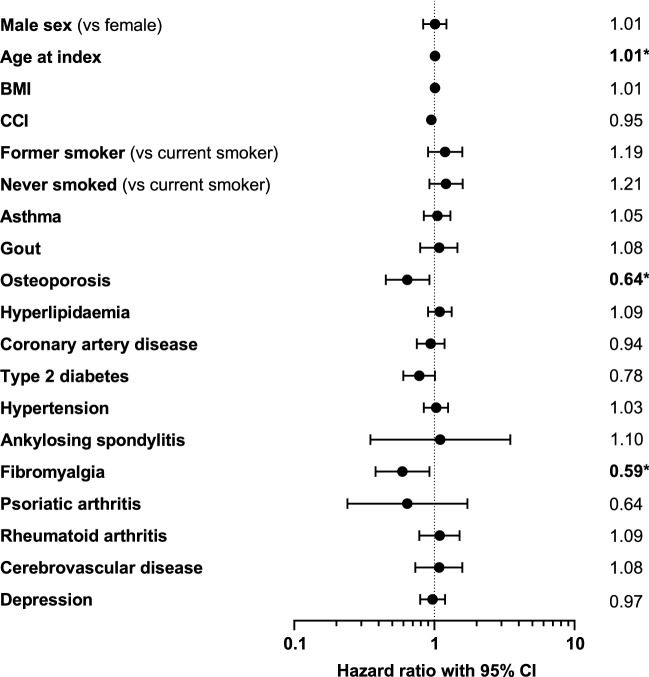
The M-S OA pain and control cohorts each comprised 3123 patients; the severe OA pain and control cohorts each comprised 1922 patients. Patients in both OA pain cohorts had a significantly higher mean number of general practitioner encounters, inpatient, outpatient, and accident and emergency visits, and were prescribed a broader range of analgesic drugs in the year post-index than respective controls. Mean healthcare costs of all types were significantly higher in the M-S and severe OA pain cohorts vs controls (total: M-S £2519 vs £1379; severe £3389 vs £1397). Paracetamol (M-S: 40% of patients had at least one prescription; severe: 50%) and strong opioids (34% and 59%) were the analgesics most prescribed to patients with OA pain. In all cohorts, multivariable models showed that a higher age at index, the presence of gout, osteoporosis, type 2 diabetes, or coronary artery disease, significantly contributed towards higher healthcare costs.
In the population of Salford, UK, patients with M-S OA pain had significantly higher annual HCRU and costs compared with matched controls without OA; generally, these were even higher in patients with severe OA pain.
利用来自英国索尔福德患者的数据,我们旨在比较中重度或重度骨关节炎(OA)疼痛患者与无OA患者之间的医疗资源利用(HCRU)和直接医疗成本。
2010年至2017年间,从索尔福德综合记录(SIR)中索引出慢性疼痛期内发生中重度OA疼痛事件的患者。发生严重疼痛事件的患者组成OA亚队列。每个OA疼痛队列中的患者与无OA患者独立匹配,形成两个对照队列。计算索引后一年的HCRU、处方镇痛药以及按英国标准化关税计算的总直接成本。使用多变量模型来确定医疗成本的驱动因素。
中重度OA疼痛队列和对照队列各有3123名患者;重度OA疼痛队列和对照队列各有1922名患者。两个OA疼痛队列中的患者在索引后一年的全科医生就诊、住院、门诊和急诊就诊的平均次数均显著更高,并且处方的镇痛药种类比各自的对照组更广泛。中重度和重度OA疼痛队列的所有类型的平均医疗成本均显著高于对照组(总计:中重度2519英镑对1379英镑;重度3389英镑对1397英镑)。对乙酰氨基酚(中重度:40%的患者至少有一张处方;重度:50%)和强阿片类药物(34%和59%)是最常开给OA疼痛患者的镇痛药。在所有队列中,多变量模型显示,索引时年龄较大、患有痛风、骨质疏松症、2型糖尿病或冠状动脉疾病,显著导致更高的医疗成本。
在英国索尔福德的人群中,与匹配的无OA对照相比,中重度OA疼痛患者的年度HCRU和成本显著更高;一般来说,重度OA疼痛患者的这些指标甚至更高。