Kishlyansky David, Kline Gregory, Mahajan Amita, Koro Konstantin, Pasieka Janice L, Champagne Patrick
Division of Internal Medicine, Department of Medicine, University of Calgary, Calgary, Alberta, Canada.
Divison of Endocrinology and Metabolism, Department of Medicine, University of Calgary, Calgary, Alberta, Canada.
Endocrinol Diabetes Metab Case Rep. 2022 Mar 1;2022. doi: 10.1530/EDM-21-0189.
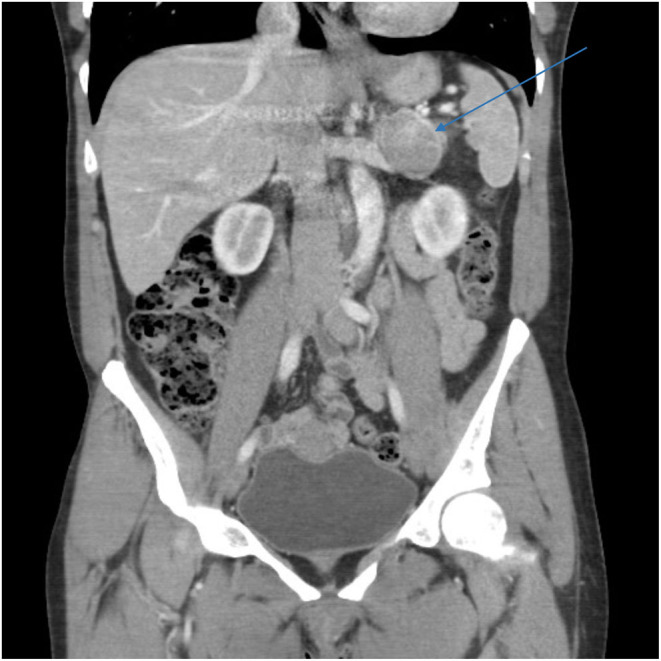
An adrenocorticotropic hormone (ACTH)-producing pheochromocytoma (PCC)/paraganglioma is the cause of ectopic Cushing's syndrome (CS) in 5.2% of cases reported in the literature. We present a previously healthy 43-year-old woman admitted to our hospital with cushingoid features and hypertensive urgency (blood pressure = 200/120 mmHg). Her 24-h urinary free cortisol was >4270 nmol/day (reference range (RR) = 100-380 nmol/day) with a plasma ACTH of 91.5 pmol/L (RR: 2.0-11.5 pmol/L). Twenty-four-hour urinary metanephrines were increased by 30-fold. Whole-body CT demonstrated a 3.7-cm left adrenal mass with a normal-appearing right adrenal gland. Sellar MRI showed a 5-mm sellar lesion. MIBG scan revealed intense uptake only in the left adrenal mass. She was managed pre-operatively with ketoconazole and phenoxybenzamine and underwent an uneventful left laparoscopic adrenalectomy, which resulted in biochemical resolution of her hypercortisolemia and catecholamine excess. Histology demonstrated a PCC (Grading System for Adrenal Pheochromocytoma and Paraganglioma score 5) with positive ACTH staining by immunohistochemistry. A PCC gene panel showed no mutations and there has been no evidence of recurrence at 24 months. This case highlights the difficult nature of localizing the source of CS in the setting of a co-existing PCC and sellar mass.
An adrenocorticotropic hormone (ACTH)-producing pheochromocytoma (PCC) is an important item to be considered in all patients presenting with ectopic Cushing's syndrome (CS). In exceptionally rare cases, patients with ectopic CS may present with multiple lesions, and a systematic approach considering all potential sources is crucial to avoid misdiagnosis. CS with a large adrenal mass but lacking contralateral adrenal atrophy should raise suspicion of an ACTH-dependent process. In patients with clinical suspicion of PCC, clinicians should be mindful of the use of steroids and beta-blockers without appropriate alpha blockade as they may precipitate an adrenergic crisis.
分泌促肾上腺皮质激素(ACTH)的嗜铬细胞瘤(PCC)/副神经节瘤是文献报道的异位库欣综合征(CS)病例中5.2%的病因。我们报告一名43岁既往健康的女性因库欣样特征和高血压急症(血压=200/120 mmHg)入院。她的24小时尿游离皮质醇>4270 nmol/天(参考范围(RR)=100 - 380 nmol/天),血浆ACTH为91.5 pmol/L(RR:2.0 - 11.5 pmol/L)。24小时尿间甲肾上腺素增加了30倍。全身CT显示左肾上腺有一个3.7厘米的肿块,右侧肾上腺外观正常。蝶鞍MRI显示一个5毫米的蝶鞍病变。MIBG扫描仅显示左肾上腺肿块有强烈摄取。她术前接受酮康唑和酚苄明治疗,随后顺利进行了腹腔镜左肾上腺切除术,术后高皮质醇血症和儿茶酚胺过量的生化指标恢复正常。组织学显示为嗜铬细胞瘤(肾上腺嗜铬细胞瘤和副神经节瘤分级系统评分为5),免疫组化显示ACTH染色阳性。PCC基因检测未发现突变,24个月时无复发迹象。该病例突出了在并存PCC和蝶鞍肿块的情况下定位CS来源的困难。
分泌促肾上腺皮质激素(ACTH)的嗜铬细胞瘤(PCC)是所有表现为异位库欣综合征(CS)患者都应考虑的重要因素。在极为罕见的情况下,异位CS患者可能出现多个病变,采用考虑所有潜在来源的系统方法对于避免误诊至关重要。有大肾上腺肿块但缺乏对侧肾上腺萎缩的CS应怀疑为ACTH依赖性过程。对于临床怀疑有PCC的患者,临床医生应注意在没有适当α受体阻滞的情况下使用类固醇和β受体阻滞剂,因为它们可能引发肾上腺素能危象。