Department of Obstetrics and Gynecology, Nagoya University Graduate School of Medicine, Nagoya, Japan.
J Gynecol Oncol. 2022 Jul;33(4):e40. doi: 10.3802/jgo.2022.33.e40. Epub 2022 Feb 21.
The survival benefits of retroperitoneal lymphadenectomy (RLNA) for epithelial ovarian cancer (EOC) remain controversial because clinical behaviors differ among subtypes. The purpose of the present study was to clarify whether RLNA increases the survival rate of advanced high-grade serous carcinoma (HGSC).
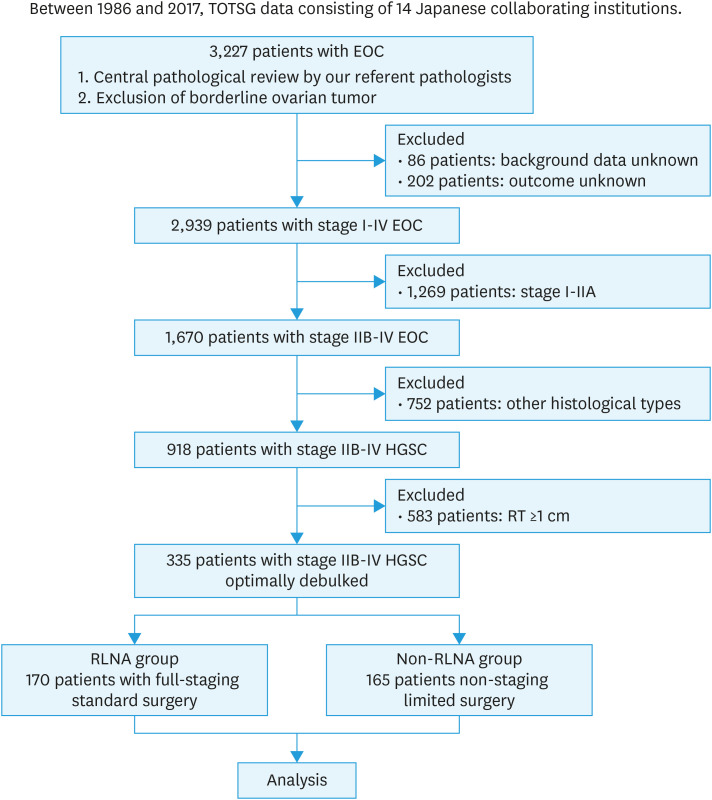
This was a retrospective cohort analysis of 3,227 patients with EOC treated between 1986 and 2017 at 14 institutions. Among them, 335 patients with stage IIB-IV HGSC who underwent optimal cytoreduction (residual tumor of <1 cm) were included. Patients were divided into the RLNA group (n=170) and non-RLNA group (n=165). All pathological slides were assessed based on a central pathological review. Oncologic outcomes were compared between the two groups in the original and weighted cohorts adjusted with the inverse probability of treatment weighting.
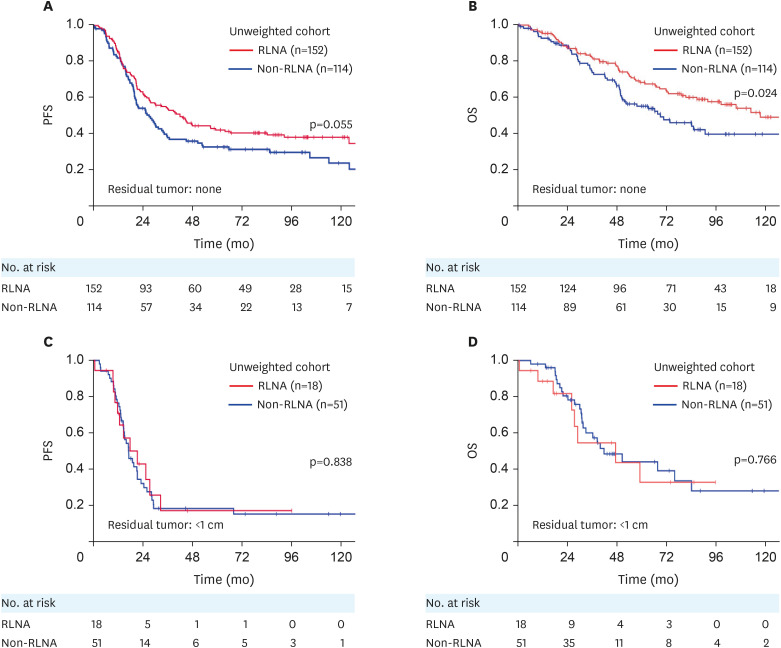
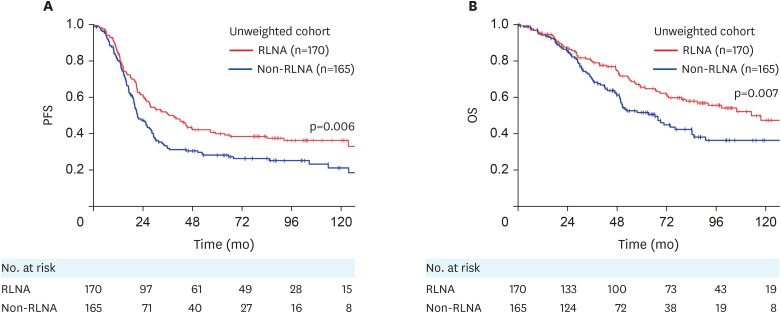
The median observation period was 49.8 (0.5-241.5) months. Overall, 219 (65%) out of 335 patients had recurrence or progression, while 146 (44%) died of the disease. In the original cohort, RLNA was a significant prognostic factor for longer progression-free survival (PFS) (hazard ratio [HR]=0.741; 95% confidence interval [CI]=0.558-0.985) and overall survival (OS) (HR=0.652; 95% CI=0.459-0.927). In the weighted cohort in which all variables were well balanced as standardized differences decreased, RLNA was also a significant prognostic factor for more favorable oncologic outcomes (PFS, adjusted HR=0.742; 95% CI=0.613-0.899) and OS, adjusted HR=0.620; 95% CI=0.488-0.787).
The present study demonstrated that RLNA for stage III-IV HGSC with no residual tumor after primary debulking surgery contributed to better oncologic outcomes.
腹膜后淋巴结清扫术(RLNA)对上皮性卵巢癌(EOC)的生存获益仍存在争议,因为不同亚型的临床行为存在差异。本研究旨在阐明 RLNA 是否能提高晚期高级别浆液性癌(HGSC)的生存率。
这是一项回顾性队列分析,纳入了 1986 年至 2017 年在 14 家机构接受治疗的 3227 名 EOC 患者。其中,335 名接受了最佳减瘤术(残余肿瘤<1cm)的 IIB-IV 期 HGSC 患者被纳入研究。患者被分为 RLNA 组(n=170)和非 RLNA 组(n=165)。所有病理切片均基于中心病理评估。在原始队列和加权队列中,通过治疗反概率加权调整后,比较两组的肿瘤学结局。
中位观察期为 49.8(0.5-241.5)个月。总体而言,335 名患者中有 219 名(65%)出现复发或进展,146 名(44%)死于该病。在原始队列中,RLNA 是无复发生存期(PFS)(风险比[HR]=0.741;95%置信区间[CI]=0.558-0.985)和总生存期(OS)(HR=0.652;95% CI=0.459-0.927)更长的显著预后因素。在加权队列中,所有变量均得到很好的平衡,标准化差异降低,RLNA 也是更好的肿瘤学结局(PFS,调整 HR=0.742;95% CI=0.613-0.899)和 OS,调整 HR=0.620;95% CI=0.488-0.787)的显著预后因素。
本研究表明,对于原发性减瘤术后无残留肿瘤的 III-IV 期 HGSC,进行 RLNA 有助于获得更好的肿瘤学结局。