Chan J K, Urban R, Hu J M, Shin J Y, Husain A, Teng N N, Berek J S, Osann K, Kapp D S
Division of Gynecologic Oncology, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of California, San Francisco School of Medicine, 1600 Divisadero Street, Box 1702, San Francisco, CA 94143, USA.
Br J Cancer. 2007 Jun 18;96(12):1817-22. doi: 10.1038/sj.bjc.6603803. Epub 2007 May 22.
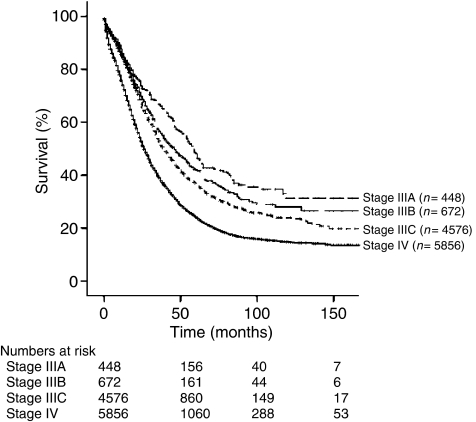
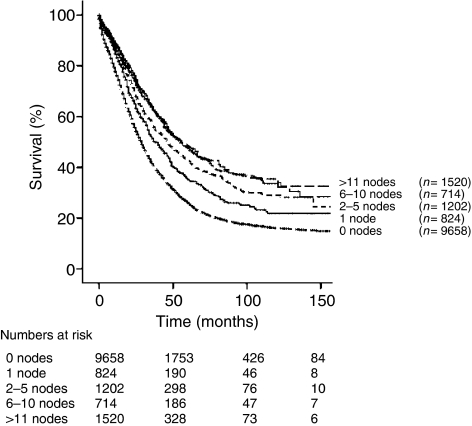
The aim of the study is to determine the role of lymphadenectomy in advanced epithelial ovarian cancer. The data were obtained from the Surveillance, Epidemiology and End Results (SEER) program reported between 1988 and 2001. Kaplan-Meier estimates and Cox proportional hazards regression models were used for analysis. Of 13 918 women with stage III-IV epithelial ovarian cancer (median age: 64 years), 87.9% were Caucasian, 5.6% African Americans, and 4.4% Asians. A total of 4260 (30.6%) underwent lymph node dissections with a median number of six nodes reported. For all patients, a more extensive lymph node dissection (0, 1, 2-5, 6-10, 11-20, and >20 nodes) was associated with an improved 5-year disease-specific survival of 26.1, 35.2, 42.6, 48.4, 47.5, and 47.8%, respectively (P<0.001). Of the stage IIIC patients with nodal metastases, the extent of nodal resection (1, 2-5, 6-10, 11-20, and >20 nodes) was associated with improved survivals of 36.9, 45.0, 47.8, 48.7, and 51.1%, respectively (P=0.023). On multivariate analysis, the extent of lymph node dissection and number of positive nodes were significant independent prognosticators after adjusting for age, year at diagnosis, stage, and grade of disease. The extent of lymphadenectomy is associated with an improved disease-specific survival of women with advanced epithelial ovarian cancer.
本研究的目的是确定淋巴结切除术在晚期上皮性卵巢癌中的作用。数据来源于1988年至2001年报告的监测、流行病学和最终结果(SEER)计划。采用Kaplan-Meier估计法和Cox比例风险回归模型进行分析。在13918例III-IV期上皮性卵巢癌女性患者中(中位年龄:64岁),87.9%为白种人,5.6%为非裔美国人,4.4%为亚洲人。共有4260例(30.6%)患者接受了淋巴结清扫术,报告的淋巴结中位数为6个。对于所有患者,更广泛的淋巴结清扫(0、1、2-5、6-10、11-20和>20个淋巴结)分别与5年疾病特异性生存率提高26.1%、35.2%、42.6%、48.4%、47.5%和47.8%相关(P<0.001)。在有淋巴结转移的IIIC期患者中,淋巴结切除范围(1、2-5、6-10、11-20和>20个淋巴结)分别与生存率提高36.9%、45.0%、47.8%、48.7%和51.1%相关(P=0.023)。多因素分析显示,在调整年龄、诊断年份、分期和疾病分级后,淋巴结清扫范围和阳性淋巴结数量是显著的独立预后因素。淋巴结切除术的范围与晚期上皮性卵巢癌女性患者的疾病特异性生存率提高相关。