Department of Renal Medicine and The Clinic of Hypertension Aarhus University Hospital Denmark.
Department of Clinical Medicine Aarhus University Denmark.
J Am Heart Assoc. 2022 Apr 5;11(7):e024421. doi: 10.1161/JAHA.121.024421. Epub 2022 Mar 24.
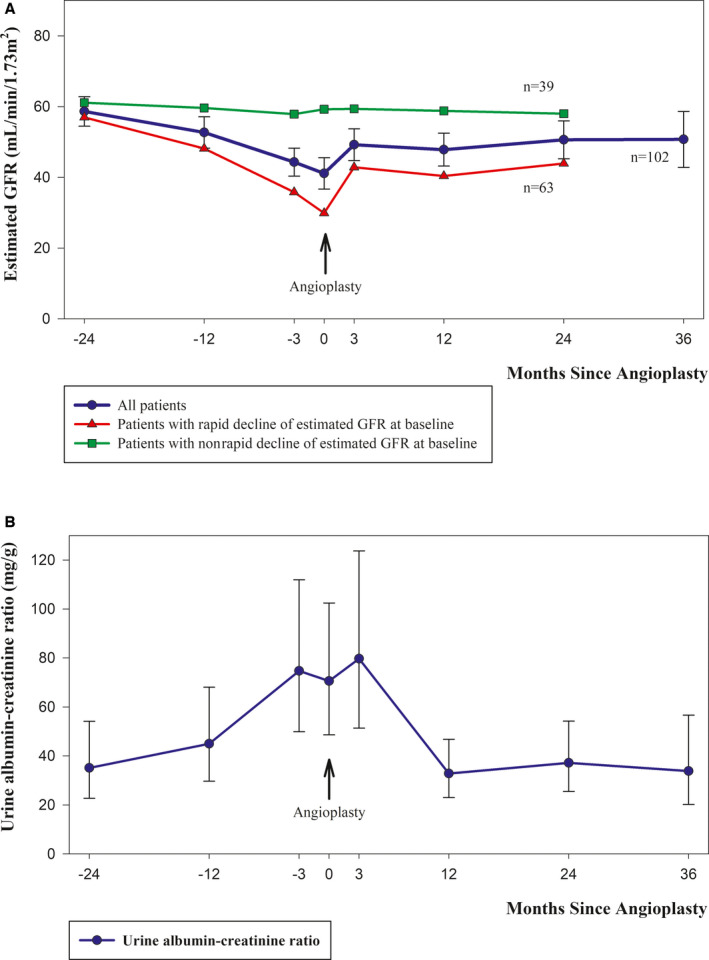
Background The aim of this study was to prospectively evaluate the effects of renal artery stenting in consecutive patients with severe atherosclerotic renal artery stenosis and high-risk clinical presentations as defined in a national protocol developed in 2015. Methods and Results Since the protocol was initiated, 102 patients have been referred for revascularization according to the following high-risk criteria: severe renal artery stenosis (≥70%) with true resistant hypertension, rapidly declining kidney function, or recurrent heart failure/sudden pulmonary edema. At baseline, the mean 24-hour ambulatory systolic blood pressure was 166.2 mm Hg (95% CI, 162.0-170.4), the defined daily dose of antihypertensive medication was 6.5 (95% CI, 5.8-7.3), and the estimated glomerular filtration rate was 41.1 mL/min per 1.73m (95% CI, 36.6-45.6). In 96 patients with available 3-month follow-up data, mean 24-hour ambulatory systolic blood pressure decreased by 19.6 mm Hg (95% CI, 15.4-23.8; 0.001), the defined daily dose of antihypertensive medication was reduced by 52% (95% CI, 41%-62%; <0.001), and estimated glomerular filtration rate increased by 7.8 mL/min per 1.73m (95% CI, 4.5-11.1; <0.001). All changes persisted after 24 month follow-up. Among 17 patients with a history of hospitalization for acute decompensated heart failure, 14 patients had no new episodes after successful revascularization. Conclusions In this prospective cohort study, we observed a reduction in blood pressure and antihypertensive medication, an increase in estimated glomerular filtration rate, and a decrease in new hospital admissions attributable to heart failure/sudden pulmonary edema after renal artery stenting. Registration URL: https://clinicaltrials.gov. Identifier: NCT02770066.
背景 本研究旨在前瞻性评估在 2015 年制定的国家方案中定义的高危临床表现的严重粥样硬化性肾动脉狭窄连续患者中进行肾动脉支架置入术的效果。
方法和结果 自该方案启动以来,根据以下高危标准将 102 例患者转诊进行血运重建:严重肾动脉狭窄(≥70%)伴真性难治性高血压、肾功能迅速下降或复发性心力衰竭/突发性肺水肿。基线时,24 小时动态收缩压平均值为 166.2mmHg(95%CI,162.0-170.4),抗高血压药物的定义日剂量为 6.5(95%CI,5.8-7.3),估计肾小球滤过率为 41.1mL/min/1.73m(95%CI,36.6-45.6)。在 96 例有 3 个月随访数据的患者中,24 小时动态收缩压平均下降 19.6mmHg(95%CI,15.4-23.8;0.001),抗高血压药物的定义日剂量减少 52%(95%CI,41%-62%;<0.001),估计肾小球滤过率增加 7.8mL/min/1.73m(95%CI,4.5-11.1;<0.001)。所有变化在 24 个月随访后仍然存在。在 17 例有急性失代偿性心力衰竭住院史的患者中,14 例在成功血运重建后无新的心力衰竭发作。
结论 在这项前瞻性队列研究中,我们观察到肾动脉支架置入术后血压和抗高血压药物降低、估计肾小球滤过率增加以及心力衰竭/突发性肺水肿新住院人数减少。