Canfell Oliver J, Davidson Kamila, Sullivan Clair, Eakin Elizabeth, Burton-Jones Andrew
UQ Business School, Faculty of Business, Economics and Law, The University of Queensland, St Lucia, QLD, Australia.
Centre for Health Services Research, Faculty of Medicine, The University of Queensland, Herston, QLD, Australia.
BMC Public Health. 2022 Mar 24;22(1):584. doi: 10.1186/s12889-022-12939-x.
Global action to reduce obesity prevalence requires digital transformation of the public health sector to enable precision public health (PPH). Useable data for PPH of obesity is yet to be identified, collated and appraised and there is currently no accepted approach to creating this single source of truth. This scoping review aims to address this globally generic problem by using the State of Queensland (Australia) (population > 5 million) as a use case to determine (1) availability of primary data sources usable for PPH for obesity (2) quality of identified sources (3) general implications for public health policymakers.
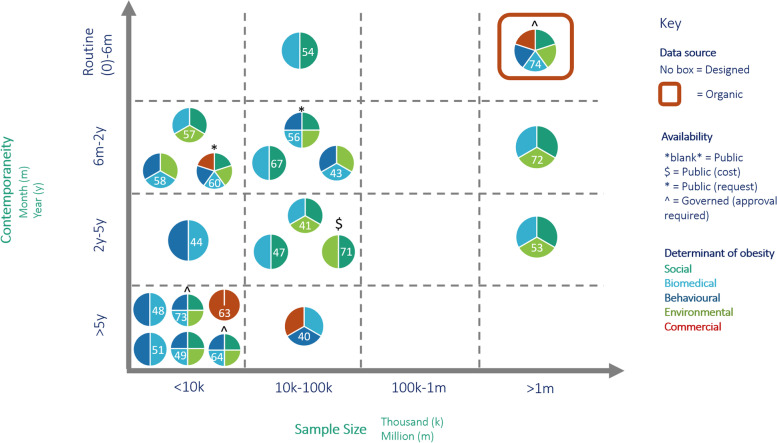
The Preferred Reporting Items for Systematic Review and Meta-Analyses extension for scoping reviews (PRISMA-ScR) was followed. Unique search strategies were implemented for 'designed' (e.g. surveys) and 'organic' (e.g. electronic health records) data sources. Only primary sources of data (with stratification to Queensland) with evidence-based determinants of obesity were included. Primary data source type, availability, sample size, frequency of collection and coverage of determinants of obesity were extracted and curated into an evidence map. Data source quality was qualitatively assessed.
We identified 38 primary sources of preventive data for obesity: 33 designed and 5 organic. Most designed sources were survey (n 20) or administrative (n 10) sources and publicly available but generally were not contemporaneous (> 2 years old) and had small sample sizes (10-100 k) relative to organic sources (> 1 M). Organic sources were identified as the electronic medical record (ieMR), wearables, environmental (Google Maps, Crime Map) and billing/claims. Data on social, biomedical and behavioural determinants of obesity typically co-occurred across sources. Environmental and commercial data was sparse and interpreted as low quality. One organic source (ieMR) was highly contemporaneous (routinely updated), had a large sample size (5 M) and represented all determinants of obesity but is not currently used for public health decision-making in Queensland.
This review provides a (1) comprehensive data map for PPH for obesity in Queensland and (2) globally translatable framework to identify, collate and appraise primary data sources to advance PPH for obesity and other noncommunicable diseases. Significant challenges must be addressed to achieve PPH, including: using designed and organic data harmoniously, digital infrastructure for high-quality organic data, and the ethical and social implications of using consumer-centred health data to improve public health.
全球减少肥胖患病率的行动需要公共卫生部门进行数字化转型,以实现精准公共卫生(PPH)。用于肥胖症精准公共卫生的可用数据尚未得到识别、整理和评估,目前也没有公认的方法来创建这一单一的真相来源。本范围综述旨在通过将昆士兰州(澳大利亚)(人口超过500万)作为一个案例,来解决这个全球普遍存在的问题,以确定(1)可用于肥胖症精准公共卫生的主要数据源的可用性;(2)已识别来源的质量;(3)对公共卫生政策制定者的一般影响。
遵循系统评价和Meta分析的首选报告项目扩展版(PRISMA-ScR)进行范围综述。针对“设计型”(如调查)和“有机型”(如电子健康记录)数据源实施了独特的搜索策略。仅纳入具有基于证据的肥胖决定因素的主要数据源(按昆士兰州分层)。提取主要数据源类型、可用性、样本量、收集频率和肥胖决定因素的覆盖范围,并整理成证据图。对数据源质量进行定性评估。
我们识别出38个肥胖预防数据的主要来源:33个设计型和5个有机型。大多数设计型来源是调查(n = 20)或行政(n = 10)来源,且可公开获取,但通常不是同期的(超过2年),相对于有机型来源(超过100万)样本量较小(10 - 100k)。有机型来源被识别为电子病历(ieMR)、可穿戴设备、环境数据(谷歌地图、犯罪地图)以及计费/理赔数据。肥胖的社会、生物医学和行为决定因素的数据通常在不同来源中同时出现。环境和商业数据稀少,被认为质量较低。一个有机型来源(ieMR)是高度同期的(定期更新),样本量很大(500万),涵盖了肥胖的所有决定因素,但目前在昆士兰州尚未用于公共卫生决策。
本综述提供了(1)昆士兰州肥胖症精准公共卫生的综合数据图,以及(2)一个全球可转化的框架,用于识别、整理和评估主要数据源,以推进肥胖症及其他非传染性疾病的精准公共卫生。要实现精准公共卫生,必须应对重大挑战,包括:和谐使用设计型和有机型数据、高质量有机数据的数字基础设施,以及使用以消费者为中心的健康数据改善公共卫生的伦理和社会影响。