Division of Pulmonology, Dept of Internal Medicine, Medical University of Graz, Graz, Austria.
Ludwig Boltzmann Institute for Lung Vascular Research, Graz, Austria.
Eur Respir J. 2022 Oct 13;60(4). doi: 10.1183/13993003.03181-2021. Print 2022 Oct.
The cardiopulmonary haemodynamic profile observed during exercise may identify patients with early-stage pulmonary vascular and primary cardiac diseases, and is used clinically to inform prognosis. However, a standardised approach to interpreting haemodynamic parameters is lacking.
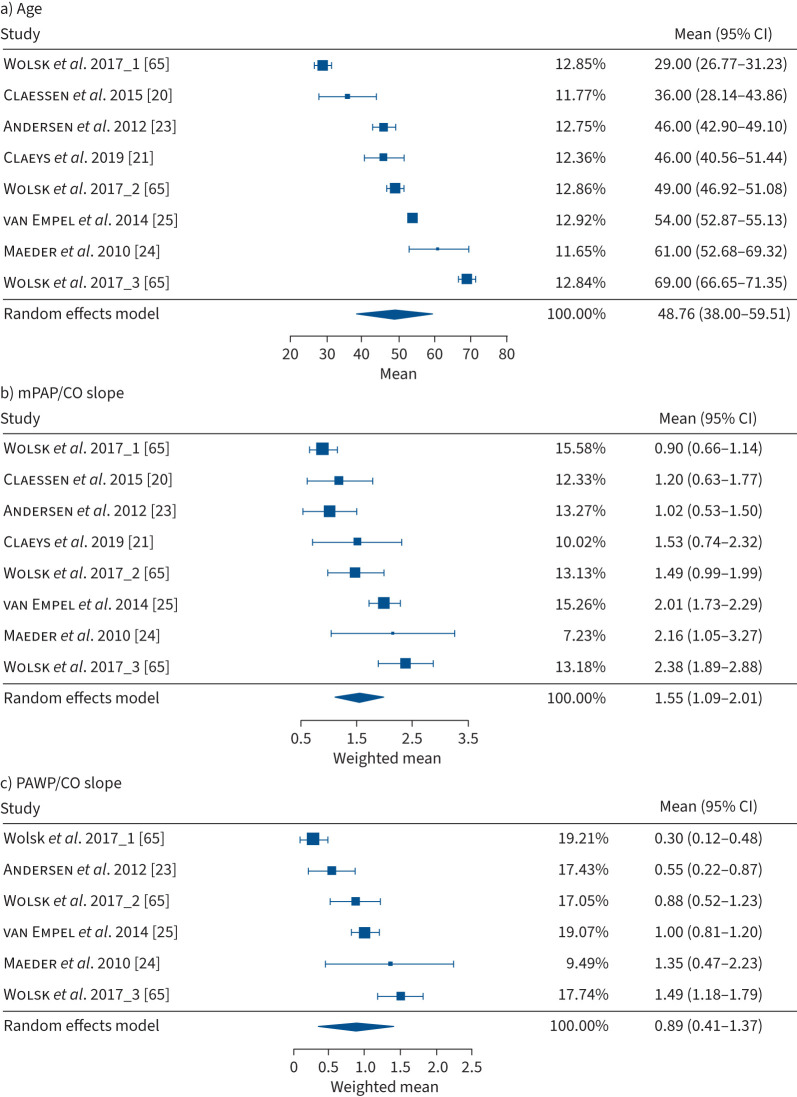
We performed a systematic literature search according to PRISMA guidelines to identify parameters that may be diagnostic for an abnormal haemodynamic response to exercise and offer optimal prognostic and differential-diagnostic value. We performed random-effects meta-analyses of the normal values and report effect sizes as weighted mean±sd. Results of diagnostic and prognostic studies are reported descriptively.
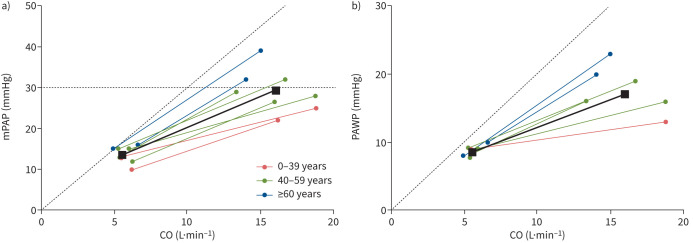
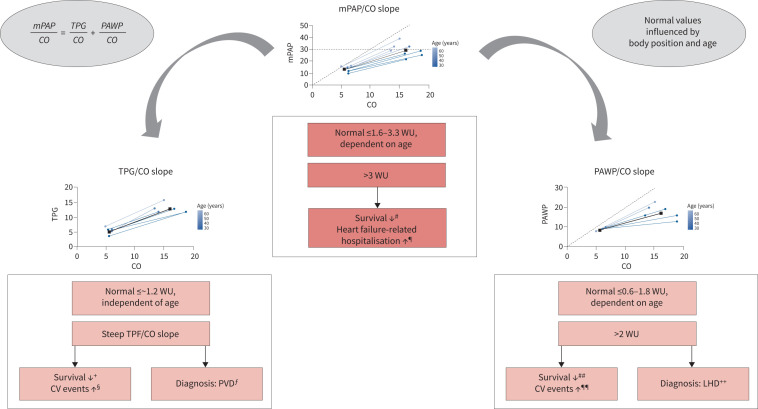
We identified 45 eligible studies with a total of 5598 subjects. The mean pulmonary arterial pressure (mPAP)/cardiac output (CO) slope, pulmonary arterial wedge pressure (PAWP)/CO slope and peak cardiac index (or CO) provided the most consistent prognostic haemodynamic parameters during exercise. The best cut-offs for survival and cardiovascular events were a mPAP/CO slope >3 Wood units (WU) and PAWP/CO slope >2 WU. A PAWP/CO slope cut-off >2 WU best differentiated pre- from post-capillary causes of PAP elevation during exercise. Upper limits of normal (defined as mean+2sd) for the mPAP/CO and PAWP/CO slopes were strongly age-dependent and ranged in 30-70-year-old healthy subjects from 1.6 to 3.3 WU and 0.6 to 1.8 WU, respectively.
An increased mPAP/CO slope during exercise is associated with impaired survival and an independent, prognostically relevant cut-off >3 WU has been validated. A PAWP/CO slope >2 WU may be suitable for the differentiation between pre- and post-capillary causes of PAP increase during exercise.
运动过程中心肺血液动力学特征可识别早期肺血管和原发性心脏疾病患者,并用于临床预测预后。然而,目前缺乏解读血液动力学参数的标准化方法。
我们按照 PRISMA 指南进行了系统文献检索,以确定可能对运动时异常血液动力学反应具有诊断意义并提供最佳预后和鉴别诊断价值的参数。我们对正常值进行了随机效应荟萃分析,并报告加权均数±标准差作为效应量。诊断和预后研究的结果以描述性方式报告。
我们确定了 45 项符合条件的研究,共纳入 5598 例受试者。运动时肺动脉平均压(mPAP)/心输出量(CO)斜率、肺动脉楔压(PAWP)/CO 斜率和峰值心指数(或 CO)是最一致的预后血液动力学参数。生存和心血管事件的最佳截断值为 mPAP/CO 斜率>3 伍德单位(WU)和 PAWP/CO 斜率>2 WU。PAWP/CO 斜率>2 WU 可最佳区分运动时 PAP 升高的前、后毛细血管原因。mPAP/CO 和 PAWP/CO 斜率的正常上限(定义为均值+2sd)强烈依赖于年龄,在 30-70 岁健康受试者中分别为 1.6-3.3 WU 和 0.6-1.8 WU。
运动时 mPAP/CO 斜率增加与生存不良相关,已验证>3 WU 的独立、具有预后相关性的截断值。PAWP/CO 斜率>2 WU 可能适用于区分运动时 PAP 升高的前、后毛细血管原因。