Department of Internal Medicine, Diabetology and Nephrology in Zabrze, Medical University of Silesia, 40-055 Katowice, Poland.
Medicina (Kaunas). 2022 Mar 7;58(3):398. doi: 10.3390/medicina58030398.
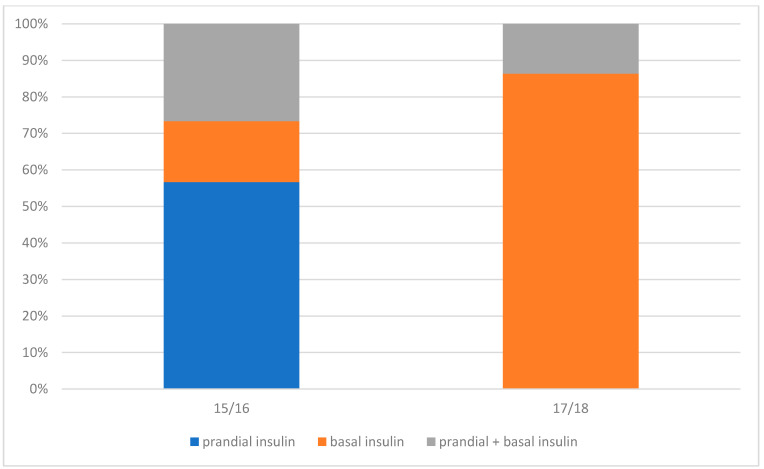
Gestational diabetes mellitus (GDM) is a significant risk factor of maternal and fetal complications. The aim of the study was to compare two groups of patients with GDM treated in 2015/2016 (Group-15/16), and in 2017/2018 (Group-17/18) and to answer the question whether the change in the diagnostic criteria for GDM affected maternal and fetal complications. : A retrospective analysis was conducted. The study included 123 patients with GDM (58 patients/Group-15/16 and 65 patients/Group-17/18). No significant differences were found between the groups. In Group-17/18, GDM was significantly more often diagnosed based on fasting glycemia (33.8%) compared with Group-15/16 (22.4%; = 0.000001). GDM was significantly more often diagnosed based on 2-h oral glucose tolerance test (OGTT; 44.8%) compared with Group-17/18 (29.2%; = 0.000005). In Group-15/16, insulin was started in 51.7% of patients compared with 33.8% in Group-17/18 ( = 0.04287). Despite more frequent insulin therapy in Group-15/16, insulin was started later (30th week of gestation) and significantly more frequently in older patients and those with higher BMI values compared with Group-17/18 (27th week of pregnancy). The number of caesarean sections and spontaneous deliveries was also similar in both periods. No difference was found in the prevalence of neonatal complications, including neonatal hypo-glycemia, prolonged jaundice or heart defect. In addition, no differences were found between the parameters in newborns. The change in the criteria for the diagnosis and treatment of GDM translated into the mode of diagnosis and currently it is more often diagnosed based on abnormal fasting glycemia. Currently, a lower percentage of patients require insulin therapy. However, less frequent inclusion of insulin may result in higher postprandial glycemia in the third trimester of pregnancy in mothers, thus increasing the risk of neonatal hypoglycemia immediately after delivery.
妊娠期糖尿病(GDM)是母婴并发症的重要危险因素。本研究旨在比较 2015/2016 年(GDM-15/16 组)和 2017/2018 年(GDM-17/18 组)两组 GDM 患者,并回答 GDM 诊断标准的改变是否影响母婴并发症。这是一项回顾性分析。研究纳入了 123 例 GDM 患者(GDM-15/16 组 58 例,GDM-17/18 组 65 例)。两组间无显著差异。GDM-17/18 组中,基于空腹血糖诊断 GDM 的比例(33.8%)明显高于 GDM-15/16 组(22.4%;=0.000001)。GDM-17/18 组中,基于 2 小时口服葡萄糖耐量试验(OGTT)诊断 GDM 的比例(44.8%)明显高于 GDM-15/16 组(29.2%;=0.000005)。GDM-15/16 组中,51.7%的患者开始使用胰岛素,而 GDM-17/18 组中这一比例为 33.8%(=0.04287)。尽管 GDM-15/16 组胰岛素治疗更频繁,但开始时间较晚(妊娠 30 周),且更常发生于年龄较大和 BMI 值较高的患者。两组间剖宫产率和自然分娩率相似。两组新生儿并发症的发生率,包括新生儿低血糖、黄疸持续时间延长或心脏缺陷,也无差异。此外,两组新生儿的参数也无差异。GDM 诊断和治疗标准的改变转化为诊断模式,目前更常基于异常空腹血糖进行诊断。目前,需要胰岛素治疗的患者比例较低。然而,较少使用胰岛素可能导致母亲妊娠晚期餐后血糖升高,从而增加新生儿出生后立即发生低血糖的风险。