Division of Emergency Medicine, Department of Medicine, University of Toronto, Toronto, ON, Canada.
Department of Emergency Medicine, University Health Network, Toronto, ON, Canada.
CJEM. 2022 Jun;24(4):382-389. doi: 10.1007/s43678-022-00280-6. Epub 2022 Mar 26.
During the COVID-19 pandemic in Ontario, Canada, an Emergency Standard of Care for Major Surge was created to establish a uniform process for the "triage" of finite critical care resources. This proposed departure from usual clinical care highlighted the need for an educational tool to prepare physicians for making and communicating difficult triage decisions. We created a just-in-time, virtual, simulation-based curriculum and evaluated its impact for our group of academic Emergency Physicians.
Our curriculum was developed and evaluated following Stufflebeam's Context-Input-Process-Product model. Our virtual simulation sessions, delivered online using Microsoft Teams, addressed a range of clinical scenarios involving decisions about critical care prioritization (i.e., Triage). Simulation participants completed a pre-course multiple-choice knowledge test and rating scales pertaining to their attitudes about using the Emergency Standard of Care protocol before and 2-4 weeks after participating. Qualitative feedback about the curriculum was solicited through surveys.
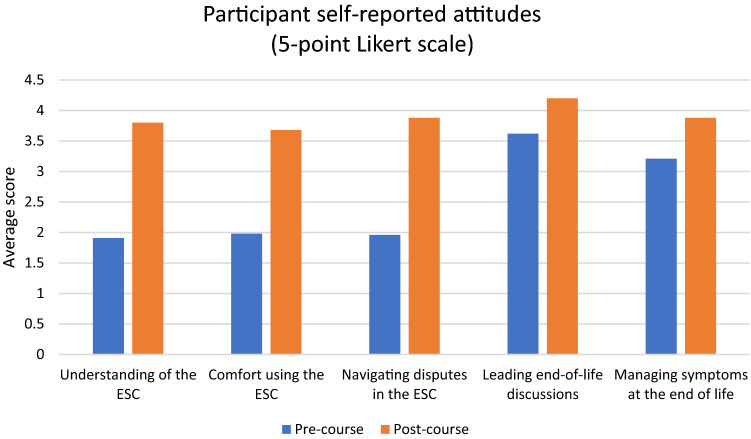
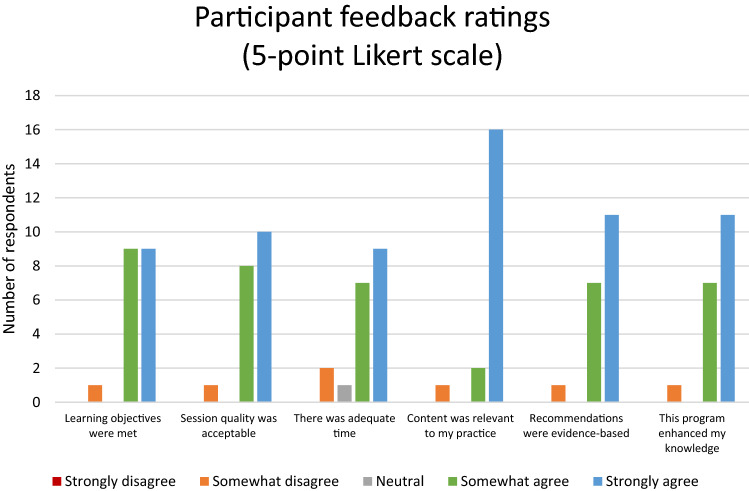
Nine virtual simulation sessions were delivered over 3 weeks, reaching a total of 47 attending emergency physicians (74% of our active department members). Overall, our intervention led to a 36% (95% CI 22.9-48.3%) improvement in participants' self-rated comfort and attitudes in navigating triage decisions and communicating with patients at the end of life. Scores on the knowledge test improved by 13% (95% CI 0.4-25.6%). 95% of participants provided highly favorable ratings of the course content and similarly indicated that the session was likely or very likely to change their practice. The curriculum has since been adopted at multiple sites around the province.
Our novel virtual simulation curriculum facilitated rapid dissemination of the Emergency Standard of Care for Major Surge to our group of Emergency Physicians despite COVID-19-related constraints on gathering. The active learning afforded by this method improved physician confidence and knowledge with these difficult protocols.
在加拿大安大略省 COVID-19 大流行期间,制定了一项重大激增紧急标准护理,以建立有限重症监护资源“分诊”的统一流程。这种偏离常规临床护理的做法突显了需要一种教育工具,为医生制定和传达困难的分诊决策做好准备。我们创建了一个即时、虚拟、基于模拟的课程,并评估了其对我们这群急诊医生的影响。
我们的课程是根据 Stufflebeam 的上下文-输入-过程-产品模型开发和评估的。我们的虚拟模拟课程通过使用 Microsoft Teams 在线提供,涉及一系列涉及重症监护优先级决策(即分诊)的临床场景。模拟参与者在参加课程之前和 2-4 周后完成了一次课前多项选择知识测试和与使用紧急标准护理协议相关的态度评定量表。通过问卷调查征求了对课程的定性反馈。
在 3 周内共进行了 9 次虚拟模拟课程,共有 47 名主治急诊医生(占我们在职部门成员的 74%)参加。总体而言,我们的干预措施使参与者在导航分诊决策和与临终患者沟通方面的自我舒适度和态度提高了 36%(95%CI 22.9-48.3%)。知识测试的分数提高了 13%(95%CI 0.4-25.6%)。95%的参与者对课程内容给予高度好评,并同样表示该课程很可能或非常可能改变他们的实践。该课程已在该省的多个地点采用。
尽管 COVID-19 限制了聚集,但我们新颖的虚拟模拟课程仍能快速向我们的急诊医生群体传播重大激增紧急标准护理。这种主动学习方法提高了医生对这些困难协议的信心和知识。