Department of Parasitology, National Institute for Medical Research, Mwanza Medical Research Centre, Mwanza, Tanzania.
School of Epidemiology and Public Health, University of Ottawa, Ottawa, ON, Canada.
Lancet. 2022 Mar 26;399(10331):1227-1241. doi: 10.1016/S0140-6736(21)02499-5.
Long-lasting insecticidal nets (LLINs) have successfully reduced malaria in sub-Saharan Africa, but their effectiveness is now partly compromised by widespread resistance to insecticides among vectors. We evaluated new classes of LLINs with two active ingredients with differing modes of action against resistant malaria vectors.
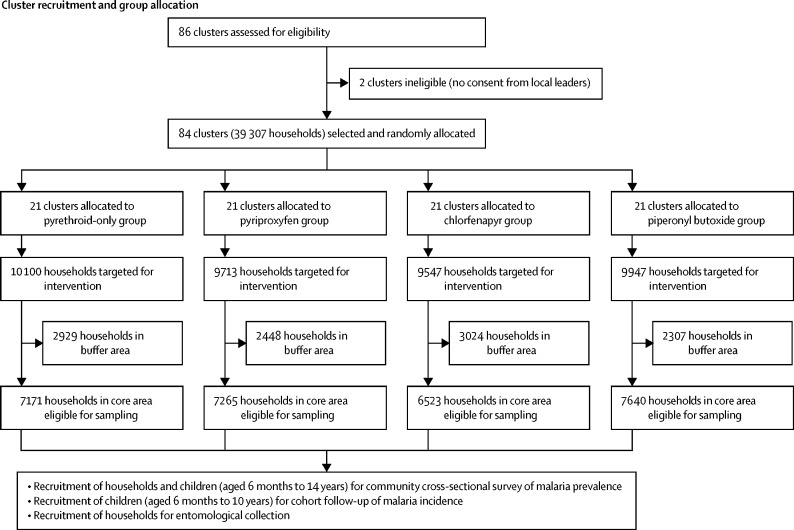
We did a four-arm, cluster-randomised trial in Misungwi, Tanzania. Clusters were villages, or groups of hamlets, with at least 119 households containing children aged 6 months to 14 years living in the cluster's core area. Constrained randomisation was used to allocate clusters (1:1:1:1) to receive one of four types of LLIN treated with the following: α-cypermethrin only (pyrethroid-only [reference] group); pyriproxyfen and α-cypermethrin (pyriproxyfen group); chlorfenapyr and α-cypermethrin (chlorfenapyr group); or the synergist piperonyl butoxide and permethrin (piperonyl butoxide group). At least one LLIN was distributed for every two people. Community members and the field team were masked to group allocation. Malaria prevalence data were collected through cross-sectional surveys of randomly selected households from each cluster, in which children aged 6 months to 14 years were assessed for Plasmodium falciparum malaria infection by rapid diagnostic tests. The primary outcome was malaria infection prevalence at 24 months after LLIN distribution, comparing each of the dual-active-ingredient LLINs to the standard pyrethroid-only LLINs in the intention-to-treat population. The primary economic outcome was cost-effectiveness of dual-active-ingredient LLINs, based on incremental cost per disability-adjusted life-year (DALY) averted compared with pyrethroid-only LLINs, modelled over a 2-year period; we included costs of net procurement and malaria diagnosis and treatment, and estimated DALYs in all age groups. This study is registered with ClinicalTrials.gov (NCT03554616), and is ongoing but no longer recruiting.
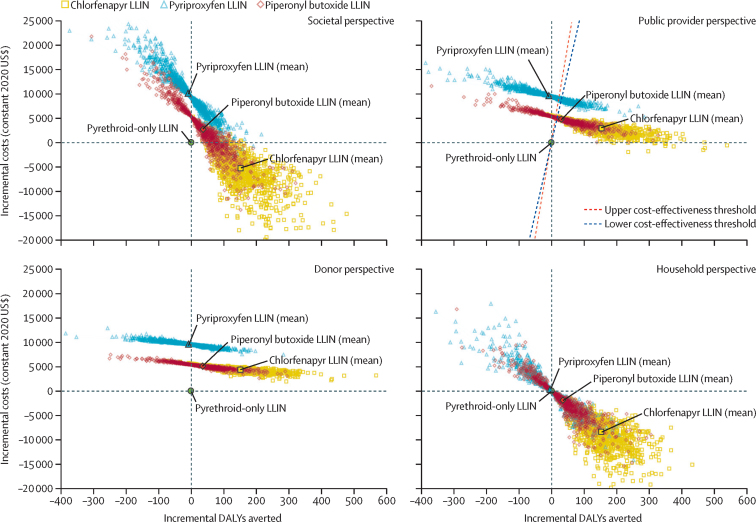
84 clusters comprising 39 307 households were included in the study between May 11 and July 2, 2018. 147 230 LLINs were distributed among households between Jan 26 and Jan 28, 2019. Use of study LLINs was reported in 3155 (72·1%) of 4378 participants surveyed at 3 months post-distribution and decreased to 8694 (40·9%) of 21 246 at 24 months, with varying rates of decline between groups. Malaria infection prevalence at 24 months was 549 (45·8%) of 1199 children in the pyrethroid-only reference group, 472 (37·5%) of 1258 in the pyriproxyfen group (adjusted odds ratio 0·79 [95% CI 0·54-1·17], p=0·2354), 512 (40·7%) of 1259 in the piperonyl butoxide group (0·99 [0·67-1·45], p=0·9607), and 326 [25·6%] of 1272 in the chlorfenapyr group (0·45 [0·30-0·67], p=0·0001). Skin irritation or paraesthesia was the most commonly reported side-effect in all groups. Chlorfenapyr LLINs were the most cost-effective LLINs, costing only US$19 (95% uncertainty interval 1-105) more to public providers or $28 (11-120) more to donors per DALY averted over a 2-year period compared with pyrethroid-only LLINs, and saving costs from societal and household perspectives.
After 2 years, chlorfenapyr LLINs provided significantly better protection than pyrethroid-only LLINs against malaria in an area with pyrethroid-resistant mosquitoes, and the additional cost of these nets would be considerably below plausible cost-effectiveness thresholds ($292-393 per DALY averted). Before scale-up of chlorfenapyr LLINs, resistance management strategies are needed to preserve their effectiveness. Poor textile and active ingredient durability in the piperonyl butoxide and pyriproxyfen LLINs might have contributed to their relative lack of effectiveness compared with standard LLINs.
Joint Global Health Trials scheme (UK Foreign, Commonwealth and Development Office; UK Medical Research Council; Wellcome; UK Department of Health and Social Care), US Agency for International Development, President's Malaria Initiative.
长效杀虫蚊帐(LLINs)在撒哈拉以南非洲成功降低了疟疾发病率,但由于病媒对杀虫剂的广泛耐药性,其效果现在部分受到影响。我们评估了两种具有不同作用模式的新型 LLINs,用于对抗具有抗药性的疟疾病媒。
我们在坦桑尼亚的米松圭进行了一项为期 4 年的、包含 4 个治疗臂的、以群组为单位的随机对照试验。群组为村庄或小村庄群,每组至少有 119 户家庭,其中包含居住在群组中心区域的年龄在 6 个月至 14 岁之间的儿童。采用约束随机化方法,将群组(1:1:1:1)随机分配接受以下四种类型的 LLIN:仅含 α-氯氰菊酯(拟除虫菊酯[参照]组);含吡丙醚和 α-氯氰菊酯(吡丙醚组);含氯氟醚菊酯和 α-氯氰菊酯(氯氟醚菊酯组);或增效剂增效醚和氯菊酯(增效醚组)。每两个人至少发放一个 LLIN。社区成员和现场团队对分组情况进行了盲法处理。通过对每个群组中的随机选择的家庭进行横断面调查,收集疟疾流行数据,其中对年龄在 6 个月至 14 岁的儿童进行快速诊断检测,以评估疟原虫感染情况。主要结局是在 LLIN 发放后 24 个月时的疟疾感染率,将每种双活性成分 LLIN 与标准拟除虫菊酯-only LLINs 在意向治疗人群中的比较。主要的经济学结局是双活性成分 LLINs 的成本效益,基于每避免一个残疾调整生命年(DALY)的增量成本,与拟除虫菊酯-only LLINs 相比,在 2 年内进行建模;我们包括了网采购和疟疾诊断和治疗的成本,并估计了所有年龄组的 DALYs。这项研究在 ClinicalTrials.gov(NCT03554616)上注册,目前正在进行中,但不再招募。
2018 年 5 月 11 日至 7 月 2 日,共有 84 个群组包含 39307 户家庭参与了研究。2019 年 1 月 26 日至 1 月 28 日,向家庭发放了 147230 个 LLIN。在分发后 3 个月的 3155 名(72.1%)4378 名参与者中报告了研究 LLIN 的使用情况,到 24 个月时下降到 8694 名(40.9%)21246 名,各组之间的下降速度不同。在 24 个月时,吡丙醚-only 参考组中 1199 名儿童中有 549 名(45.8%)患有疟疾感染,吡丙醚组中 1258 名中有 472 名(校正优势比 0.79 [95%CI 0.54-1.17],p=0.2354),增效醚组中 1259 名中有 512 名(0.99 [0.67-1.45],p=0.9607),氯氟醚菊酯组中 1272 名中有 326 名(25.6%)患有疟疾感染(0.45 [0.30-0.67],p=0.0001)。在所有组中,皮肤刺激或感觉异常是最常见的副作用。氯氟醚菊酯 LLINs 是最具成本效益的 LLINs,与仅含拟除虫菊酯的 LLINs 相比,公共提供者每避免一个 DALY 需要多花费 19 美元(95%置信区间 1-105),或者捐赠者需要多花费 28 美元(11-120),在 2 年内,从社会和家庭的角度来看,都可以节省成本。
在具有耐拟除虫菊酯病媒的地区,经过 2 年,氯氟醚菊酯 LLINs 比仅含拟除虫菊酯的 LLINs 提供了更好的疟疾保护,这些网的额外成本将远远低于合理的成本效益阈值(每避免一个 DALY 花费 292-393 美元)。在扩大氯氟醚菊酯 LLINs 的规模之前,需要采取抗药性管理策略来保持其有效性。增效醚和吡丙醚 LLINs 在纺织品和活性成分耐久性方面较差,可能是它们相对于标准 LLINs 缺乏有效性的原因。
联合全球卫生试验计划(英国外交、联邦和发展办公室;英国医学研究理事会;惠康基金会;英国卫生部和社会保障部),美国国际开发署,总统疟疾倡议。