Division of Neuro-Oncology, Department of Neurology and Herbert Irving Comprehensive Cancer Center, Columbia University Vagelos College of Physicians and Surgeons and NewYork-Presbyterian, New York, New York.
Hospital Universitario 12 De Octubre, Madrid, Spain.
Clin Cancer Res. 2022 Jun 1;28(11):2270-2277. doi: 10.1158/1078-0432.CCR-21-2664.
FGFR genomic alterations (amplification, mutations, and/or fusions) occur in ∼8% of gliomas, particularly FGFR1 and FGFR3. We conducted a multicenter open-label, single-arm, phase II study of a selective FGFR1-3 inhibitor, infigratinib (BGJ398), in patients with FGFR-altered recurrent gliomas.
Adults with recurrent/progressive gliomas harboring FGFR alterations received oral infigratinib 125 mg on days 1 to 21 of 28-day cycles. The primary endpoint was investigator-assessed 6-month progression-free survival (PFS) rate by Response Assessment in Neuro-Oncology criteria. Comprehensive genomic profiling was performed on available pretreatment archival tissue to explore additional molecular correlations with efficacy.
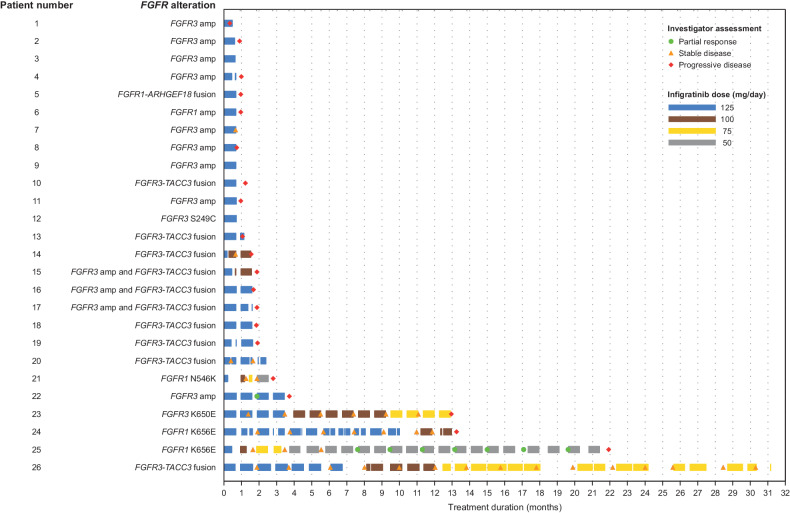
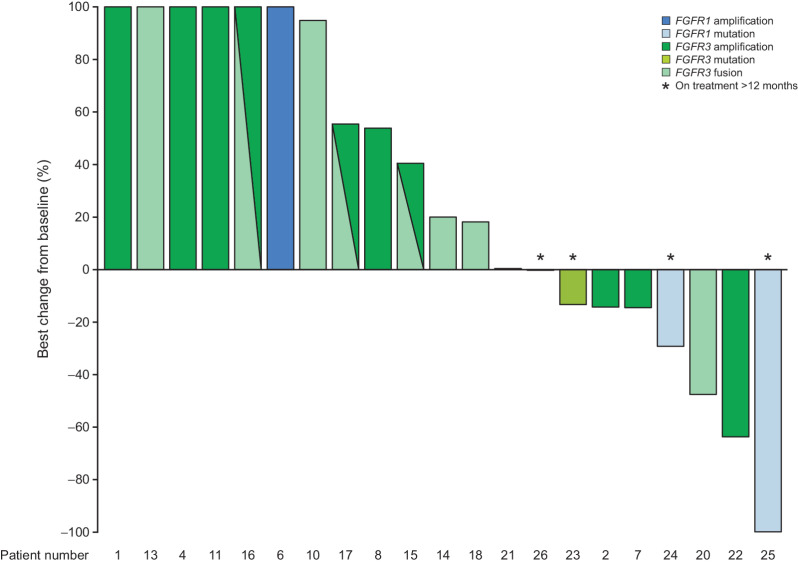
Among 26 patients, the 6-month PFS rate was 16.0% [95% confidence interval (CI), 5.0-32.5], median PFS was 1.7 months (95% CI, 1.1-2.8), and objective response rate was 3.8%. However, 4 patients had durable disease control lasting longer than 1 year. Among these, 3 had tumors harboring activating point mutations at analogous positions of FGFR1 (K656E; n = 2) or FGFR3 (K650E; n = 1) in pretreatment tissue; an FGFR3-TACC3 fusion was detected in the other. Hyperphosphatemia was the most frequently reported treatment-related adverse event (all-grade, 76.9%; grade 3, 3.8%) and is a known on-target toxicity of FGFR inhibitors.
FGFR inhibitor monotherapy with infigratinib had limited efficacy in a population of patients with recurrent gliomas and different FGFR genetic alterations, but durable disease control lasting more than 1 year was observed in patients with tumors harboring FGFR1 or FGFR3 point mutations or FGFR3-TACC3 fusions. A follow-up study with refined biomarker inclusion criteria and centralized FGFR testing is warranted.
FGFR 基因改变(扩增、突变和/或融合)发生于约 8%的胶质瘤中,特别是 FGFR1 和 FGFR3。我们进行了一项多中心、开放性、单臂、II 期研究,评估了选择性 FGFR1-3 抑制剂 infigratinib(BGJ398)在 FGFR 改变的复发性脑胶质瘤患者中的疗效。
携带 FGFR 改变的复发性/进行性脑胶质瘤患者接受口服 infigratinib 125mg,每天一次,21 天为一个周期,28 天为一个疗程。主要终点为研究者评估的根据 RECIST 标准的 6 个月无进展生存期(PFS)率。对可获得的预处理存档组织进行全面的基因组分析,以探索与疗效相关的其他分子相关性。
在 26 名患者中,6 个月的 PFS 率为 16.0%(95%CI,5.0-32.5),中位 PFS 为 1.7 个月(95%CI,1.1-2.8),客观缓解率为 3.8%。然而,有 4 名患者的疾病控制时间超过 1 年,其中 3 名患者的肿瘤在预处理组织中存在 FGFR1(K656E;n=2)或 FGFR3(K650E;n=1)的激活点突变;另 1 名患者存在 FGFR3-TACC3 融合。高磷血症是最常见的治疗相关不良事件(所有级别,76.9%;3 级,3.8%),这是 FGFR 抑制剂的已知靶点毒性。
在复发性脑胶质瘤患者中,FGFR 抑制剂单药治疗 infigratinib 的疗效有限,且存在不同的 FGFR 遗传改变,但在存在 FGFR1 或 FGFR3 点突变或 FGFR3-TACC3 融合的肿瘤患者中,观察到超过 1 年的持久疾病控制。需要进行一项后续研究,纳入更精细的生物标志物纳入标准和集中的 FGFR 检测。