Rama Tiago Azenha, Morgado José Mário, Henriques Ana, Escribano Luis, Alvarez-Twose Iván, Sanchez-Muñoz Laura, Moreira André, Romão José, Órfão Alberto, Matito Almudena
Serviço de Imunoalergologia, Centro Hospitalar Universitário São João, Porto, Portugal.
Serviço de Imunologia, Departamento de Patologia, Faculdade de Medicina da Universidade do Porto, Porto, Portugal.
Clin Transl Allergy. 2022 Mar;12(3):e12132. doi: 10.1002/clt2.12132.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are frequently avoided in mastocytosis, because of a potential increased risk for drug hypersensitivity reactions (DHRs) due to inhibition of cyclo-oxygenase (COX), subsequent depletion of prostaglandin E and release of leukotrienes.
Here, we aimed at determining the prevalence of mast cell (MC) mediator release symptoms triggered by NSAIDs in mastocytosis patients and the associated clinical and laboratory features of the disease.
Medical records from 418 adults to 223 pediatric mastocytosis patients were retrospectively reviewed. Patients were classified according to tolerance patterns to NSAIDs and other COX inhibitors (COXi) and compared for epidemiological, clinical and laboratory findings.
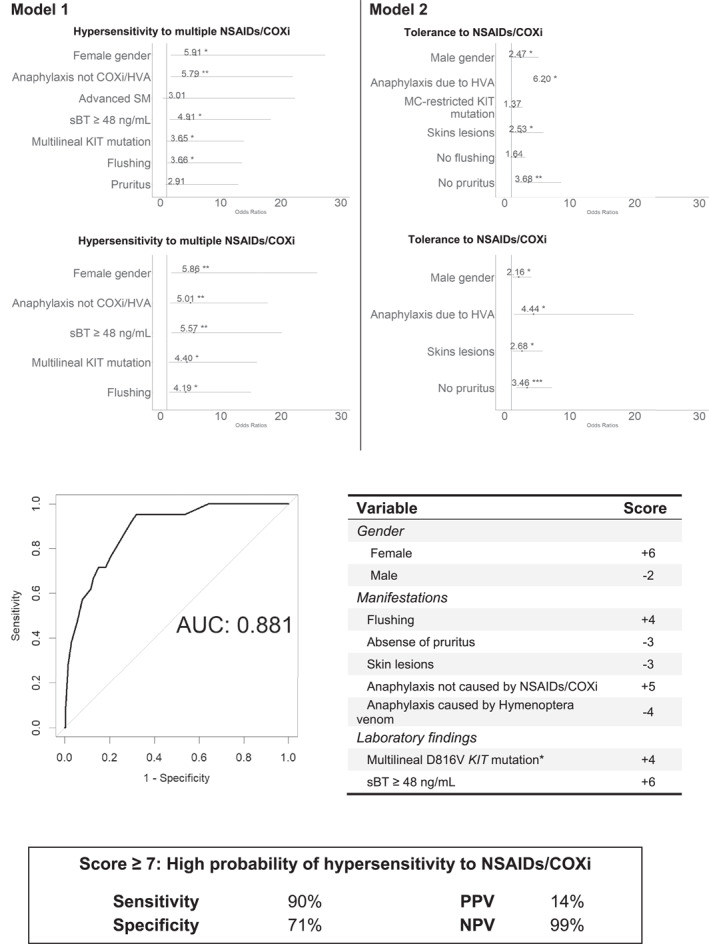
Overall, 87% of adults and 91% of pediatric patients tolerated NSAIDs and other COXi. Among adult and pediatric patients presenting DHRs, 5% and 0% reacted to multiple NSAIDs, 4% and 0.7% were single reactors, and 3% and 8% were single reactors with known tolerance to paracetamol but unknown tolerance to other COXi, respectively. Among adults, hypersensitivity to ≥2 drugs was more frequent among females (p = 0.009), patients with prior history of anaphylaxis to triggers other than NSAIDs or other COXi and Hymenoptera venom (p = 0.009), presence of baseline flushing (p = 0.02), baseline serum tryptase ≥48 ng/ml (p = 0.005) and multilineage KIT mutation (p = 0.02). In contrast, tolerance to NSAIDs and other COXi was more frequent among males (p = 0.02), in patients with anaphylaxis caused by Hymenoptera venom (p = 0.02), among individuals who had skin lesions due to mastocytosis (p = 0.01), and in cases that had no baseline pruritus (p = 0.006). Based on these parameters, a score model was designed to stratify mastocytosis patients who have never received NSAIDs or other COXi apart from paracetamol, according to their risk of DHR.
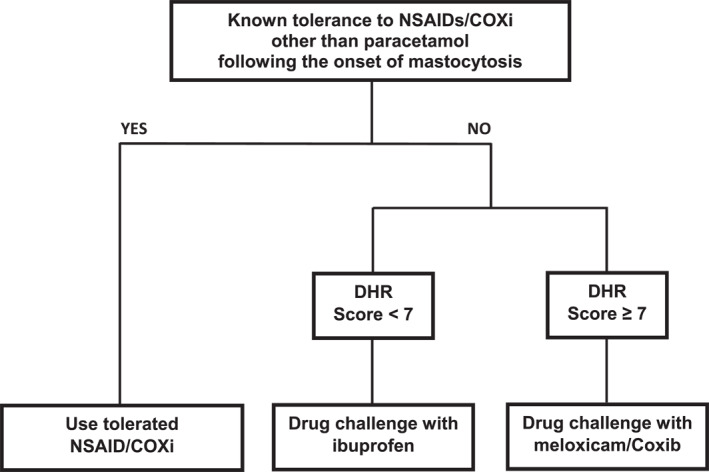
Our results suggest that despite the frequency of MC mediator related symptoms elicited by NSAIDs and other COXi apart from paracetamol is increased among mastocytosis patients versus the general population, it is lower than previously estimated and associated with unique disease features. Patients that tolerated NSAIDs and other COXi following disease onset should keep using them. In turn, adults with unknown tolerance to such drugs and a positive score should be challenged with a preferential/selective COX-2 inhibitor, while the remaining may be challenged with ibuprofen.
肥大细胞增多症患者常避免使用非甾体抗炎药(NSAIDs),因为抑制环氧化酶(COX)会导致药物过敏反应(DHRs)风险增加,进而使前列腺素E耗竭并释放白三烯。
在此,我们旨在确定肥大细胞增多症患者中由NSAIDs引发的肥大细胞(MC)介质释放症状的发生率以及该疾病相关的临床和实验室特征。
回顾性分析418例成人和223例儿童肥大细胞增多症患者的病历。根据对NSAIDs和其他COX抑制剂(COXi)的耐受模式对患者进行分类,并比较其流行病学、临床和实验室检查结果。
总体而言,87%的成人和91%的儿童患者耐受NSAIDs和其他COXi。在出现DHRs的成人和儿童患者中,分别有5%和0%对多种NSAIDs有反应,4%和0.7%为单一反应者,3%和8%为已知对扑热息痛耐受但对其他COXi耐受情况未知的单一反应者。在成人中,对≥2种药物过敏在女性中更为常见(p = 0.009),有除NSAIDs或其他COXi及膜翅目毒液以外的过敏反应既往史的患者中更为常见(p = 0.009),有基线潮红的患者中更为常见(p = 0.02),基线血清类胰蛋白酶≥48 ng/ml的患者中更为常见(p = 0.005)以及存在多谱系KIT突变的患者中更为常见(p = 0.02)。相比之下,男性对NSAIDs和其他COXi的耐受性更高(p = 0.02),由膜翅目毒液引起过敏反应的患者中更高(p = 0.02),有肥大细胞增多症所致皮肤病变的个体中更高(p = 0.01),以及无基线瘙痒的病例中更高(p = 0.006)。基于这些参数,设计了一个评分模型,用于对除扑热息痛外从未接受过NSAIDs或其他COXi的肥大细胞增多症患者根据其发生DHR的风险进行分层。
我们的结果表明,尽管与一般人群相比,肥大细胞增多症患者中由NSAIDs和除扑热息痛外的其他COXi引发的MC介质相关症状更为常见,但低于先前估计,且与独特的疾病特征相关。疾病发作后耐受NSAIDs和其他COXi的患者应继续使用。反过来,对这类药物耐受情况未知且评分阳性的成人应以优先/选择性COX - 2抑制剂进行激发试验,而其余患者可使用布洛芬进行激发试验。